Das könnte Ihnen auch gefallen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- English Time 3Dokument79 SeitenEnglish Time 3Ghadeer Ebraheem100% (2)
- One Hundred YearsDokument18 SeitenOne Hundred YearsolziichNoch keine Bewertungen
- GcsDokument1 SeiteGcsGhadeer EbraheemNoch keine Bewertungen
- ATLS DRDokument45 SeitenATLS DRNeNeei HenNieNoch keine Bewertungen
- Myotomes of The Upper LimbDokument2 SeitenMyotomes of The Upper LimbGhadeer Ebraheem0% (1)
- Usmle Surgery Mcqs PDFDokument2 SeitenUsmle Surgery Mcqs PDFGhadeer Ebraheem75% (4)
- HIV and HIV CounsellingDokument12 SeitenHIV and HIV CounsellingGhadeer EbraheemNoch keine Bewertungen
- Mansmed Surgery QbankDokument7 SeitenMansmed Surgery QbankGhadeer EbraheemNoch keine Bewertungen
- Antibody Tests (Coombs Test)Dokument2 SeitenAntibody Tests (Coombs Test)Ghadeer EbraheemNoch keine Bewertungen
- Immunoglobulin TherapyDokument5 SeitenImmunoglobulin TherapyGhadeer EbraheemNoch keine Bewertungen
- Leach and Lily Stanley - Last Updated On: Edit This Article View RevisionsDokument7 SeitenLeach and Lily Stanley - Last Updated On: Edit This Article View RevisionsGhadeer EbraheemNoch keine Bewertungen
- Leach and Lily Stanley - Last Updated On: Edit This Article View RevisionsDokument7 SeitenLeach and Lily Stanley - Last Updated On: Edit This Article View RevisionsGhadeer EbraheemNoch keine Bewertungen
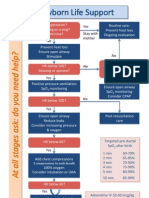
- Arc Neonatal FlowchartDokument1 SeiteArc Neonatal FlowchartChander KantaNoch keine Bewertungen
- HIV and HIV CounsellingDokument12 SeitenHIV and HIV CounsellingGhadeer EbraheemNoch keine Bewertungen
- Inflamatory Bowel Disease: Dr. Samir IsmailDokument82 SeitenInflamatory Bowel Disease: Dr. Samir IsmailGhadeer EbraheemNoch keine Bewertungen
- Acid Base PhysiologyDokument4 SeitenAcid Base PhysiologyGhadeer EbraheemNoch keine Bewertungen
- Neuro ExaminationDokument82 SeitenNeuro ExaminationGhadeer Ebraheem100% (1)
- RicketsDokument7 SeitenRicketsGhadeer EbraheemNoch keine Bewertungen
- Nephrotic SyndromeDokument1 SeiteNephrotic SyndromeGhadeer EbraheemNoch keine Bewertungen
- Vasc Med 1998 Powell 21 8Dokument9 SeitenVasc Med 1998 Powell 21 8Ghadeer EbraheemNoch keine Bewertungen
- 5 - Health Care System Awad Etc 2009Dokument11 Seiten5 - Health Care System Awad Etc 2009Ghadeer EbraheemNoch keine Bewertungen
- Anatomy 2 MnemonicsDokument46 SeitenAnatomy 2 MnemonicsGhadeer EbraheemNoch keine Bewertungen
- Drugs Causing HirsutismDokument1 SeiteDrugs Causing HirsutismGhadeer EbraheemNoch keine Bewertungen
- Drugs Causing HirsutismDokument1 SeiteDrugs Causing HirsutismGhadeer EbraheemNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)