Das könnte Ihnen auch gefallen
- Med Terminology in A Flash - CardioDokument66 SeitenMed Terminology in A Flash - CardiobencleeseNoch keine Bewertungen
- Labs Can Manipulate How Many "Cases' of Covid-19 The Country Has ' - Allan C. WDokument14 SeitenLabs Can Manipulate How Many "Cases' of Covid-19 The Country Has ' - Allan C. WrbradburyNoch keine Bewertungen
- Torque Converter Lock-Up FunctionDokument2 SeitenTorque Converter Lock-Up Functioncorie132100% (1)
- Gene Hunting: J. PongraczDokument15 SeitenGene Hunting: J. PongracztahirnaeemkhanNoch keine Bewertungen
- CSP Study Course 2 Willard StephensonDokument137 SeitenCSP Study Course 2 Willard Stephensonsamer alrawashdehNoch keine Bewertungen
- Edible Vaccines: DR Fatima Shad K Professor Panjwani Center For Molecular Medicine and Drug ResearchDokument20 SeitenEdible Vaccines: DR Fatima Shad K Professor Panjwani Center For Molecular Medicine and Drug ResearchWasim HakimNoch keine Bewertungen
- Blinded by Pseudoscience - by Mike StoneDokument21 SeitenBlinded by Pseudoscience - by Mike StoneRobert Stagnitto100% (1)
- Baric INVISIBLE Gene Editing Method For His SARS-CoV-2 JVI.76.21.11065-11078.2002Dokument14 SeitenBaric INVISIBLE Gene Editing Method For His SARS-CoV-2 JVI.76.21.11065-11078.2002Kevin SteinerNoch keine Bewertungen
- Nej M 199902113400606Dokument10 SeitenNej M 199902113400606Henra WijayaNoch keine Bewertungen
- Blood Transfusion NHMRC-Guidelines - 01Dokument113 SeitenBlood Transfusion NHMRC-Guidelines - 01Mahsa MirkazemiNoch keine Bewertungen
- "Towards Eradicating Tuberculosis" - Aetiopathogenesis of TuberculosisDokument29 Seiten"Towards Eradicating Tuberculosis" - Aetiopathogenesis of Tuberculosisibnbasheer100% (7)
- Toxicological Profile For Ionizing Radiation - ATSDRDokument438 SeitenToxicological Profile For Ionizing Radiation - ATSDRdavid_stephens_29Noch keine Bewertungen
- Biocompatibility of Graphene OxideDokument8 SeitenBiocompatibility of Graphene OxidelpuresearchNoch keine Bewertungen
- The Sourcebook for Clinical Research: A Practical Guide for Study ConductVon EverandThe Sourcebook for Clinical Research: A Practical Guide for Study ConductBewertung: 5 von 5 Sternen5/5 (1)
- Helicobacter Pylori InfectionDokument8 SeitenHelicobacter Pylori InfectionNovitaNoch keine Bewertungen
- Equine Clinical PathologyVon EverandEquine Clinical PathologyRaquel M. WaltonNoch keine Bewertungen
- Links To GoodnessDokument194 SeitenLinks To GoodnessKevin Itwaru0% (3)
- Identification of 2019-Ncov Related Coronaviruses in Malayan Pangolins in Southern ChinaDokument22 SeitenIdentification of 2019-Ncov Related Coronaviruses in Malayan Pangolins in Southern ChinaismailNoch keine Bewertungen
- Sars PDFDokument60 SeitenSars PDFVASILIS NIKNoch keine Bewertungen
- Group 7 - Mountain DewDokument18 SeitenGroup 7 - Mountain DewRishabh Anand100% (1)
- Hand Planer PDFDokument8 SeitenHand Planer PDFJelaiNoch keine Bewertungen
- Chapter 5. Intravenous InfusionDokument22 SeitenChapter 5. Intravenous InfusionbencleeseNoch keine Bewertungen
- Event Management (MAX FIT)Dokument12 SeitenEvent Management (MAX FIT)vkrish6Noch keine Bewertungen
- Covid 19 SafetyDokument8 SeitenCovid 19 SafetySargent GoodchildNoch keine Bewertungen
- Chapter 3. One-Compartment Open Model Intravenous Bolus AdministrationDokument23 SeitenChapter 3. One-Compartment Open Model Intravenous Bolus AdministrationbencleeseNoch keine Bewertungen
- Ethnic Specific Genetically Engineered WeaponsDokument135 SeitenEthnic Specific Genetically Engineered WeaponsEyemanProphetNoch keine Bewertungen
- Medical InterviewDokument12 SeitenMedical Interviewbencleese100% (1)
- Marketing Research ProjectDokument37 SeitenMarketing Research ProjectVijay100% (15)
- EMS Infectious Disease PlaybookDokument86 SeitenEMS Infectious Disease PlaybookAryttNoch keine Bewertungen
- Manual de Partes Dm45-50-lDokument690 SeitenManual de Partes Dm45-50-lklausNoch keine Bewertungen
- AIDS - The Mycoplasma EXPOSE Document PDFDokument13 SeitenAIDS - The Mycoplasma EXPOSE Document PDFPierre Le GrandeNoch keine Bewertungen
- Applied Biopharmaceutics & Pharmacokinetics, 5th EditionDokument1 SeiteApplied Biopharmaceutics & Pharmacokinetics, 5th Editionbencleese14% (7)
- Albumin InfusionDokument21 SeitenAlbumin InfusiondinniNoch keine Bewertungen
- My Conversation With State Senator and Doctor Who Exposes Medicare Payouts For COVID-19 PatientsDokument18 SeitenMy Conversation With State Senator and Doctor Who Exposes Medicare Payouts For COVID-19 PatientsNammeerNoch keine Bewertungen
- Wyeth Rotashield Package InsertDokument19 SeitenWyeth Rotashield Package InsertGeeleegoatNoch keine Bewertungen
- Statistical Analysis Linking U.S. AIDS Outbreak To Hepatitis ExperimentsDokument65 SeitenStatistical Analysis Linking U.S. AIDS Outbreak To Hepatitis Experimentsst_spyridonNoch keine Bewertungen
- Turning Nature Against ManDokument17 SeitenTurning Nature Against MantonyNoch keine Bewertungen
- Land Steiner ImpDokument4 SeitenLand Steiner ImpashokNoch keine Bewertungen
- Pi Is 1473309920307647Dokument7 SeitenPi Is 1473309920307647ZerohedgeNoch keine Bewertungen
- Allan Charles WilsonDokument2 SeitenAllan Charles WilsonAngela PageNoch keine Bewertungen
- Greed, Genocide ... and Now "Green": Corruption and Underdevelopment in GuyanaDokument22 SeitenGreed, Genocide ... and Now "Green": Corruption and Underdevelopment in GuyanaRogerWilliams100% (3)
- Parashah 15 - Bo (Go)Dokument11 SeitenParashah 15 - Bo (Go)HaSophimNoch keine Bewertungen
- COVID 19 Drug Therapy - Mar 2020 PDFDokument12 SeitenCOVID 19 Drug Therapy - Mar 2020 PDFJean-Michel Tommy Luzayamo100% (1)
- Research Essay - JessicaDokument5 SeitenResearch Essay - JessicaJessica Huerta PerezNoch keine Bewertungen
- Euthanasia CloningDokument28 SeitenEuthanasia CloningDavid RefuncionNoch keine Bewertungen
- Bloodbook 2017 660 PDFDokument7 SeitenBloodbook 2017 660 PDFSambit DashNoch keine Bewertungen
- Alien GeneDokument5 SeitenAlien GeneRashid_iqbal40@yahoo.comNoch keine Bewertungen
- 20210217-Mr G. H. Schorel-Hlavka O.W.B. To PM MR SCOTT MORRISON & Ors-Re Vaccination IssuesDokument46 Seiten20210217-Mr G. H. Schorel-Hlavka O.W.B. To PM MR SCOTT MORRISON & Ors-Re Vaccination IssuesGerrit Hendrik Schorel-HlavkaNoch keine Bewertungen
- 10 Defences For Anil Azeez Against Aksharananda's AccusationsDokument2 Seiten10 Defences For Anil Azeez Against Aksharananda's AccusationsRogerWilliamsNoch keine Bewertungen
- Novel-Coronavirus Landscape nCoV-4april2020 PDFDokument6 SeitenNovel-Coronavirus Landscape nCoV-4april2020 PDFMargaritaNoch keine Bewertungen
- 2018 01 (Jan) 11 Youtube Part 2 On 9 Stanley Plotkin, Godfather of Vaccines, UNDER OATH P. 52 To 96Dokument40 Seiten2018 01 (Jan) 11 Youtube Part 2 On 9 Stanley Plotkin, Godfather of Vaccines, UNDER OATH P. 52 To 96Jagannath100% (1)
- DR Claus Kohnlein Explains The Corona MadnessDokument1 SeiteDR Claus Kohnlein Explains The Corona MadnessCazzac111Noch keine Bewertungen
- From The Department of Medicine, Western Reserve University, ClevelandDokument31 SeitenFrom The Department of Medicine, Western Reserve University, Clevelandclarkkent2Noch keine Bewertungen
- NSABB Dismissal June2014Dokument3 SeitenNSABB Dismissal June2014kehillsNoch keine Bewertungen
- How Should We Plan For Pandemics?Dokument3 SeitenHow Should We Plan For Pandemics?Jose LopezNoch keine Bewertungen
- Exposing The Dark Side of VaccinesDokument2 SeitenExposing The Dark Side of VaccinesM. R. Wilde100% (1)
- Immreqpk15 16Dokument4 SeitenImmreqpk15 16api-234991765Noch keine Bewertungen
- Philippine Medical Association Study Indicates That Women Were Injected With Contaminated Tetanus VaccineDokument2 SeitenPhilippine Medical Association Study Indicates That Women Were Injected With Contaminated Tetanus VaccineJonathan Robert Kraus (OutofMudProductions)Noch keine Bewertungen
- A History of VaccinesDokument2 SeitenA History of VaccinesHarol CaballeroNoch keine Bewertungen
- Pa Tho Genesis and Immunology of Avian InfluenzaDokument9 SeitenPa Tho Genesis and Immunology of Avian InfluenzaHengki FerdiantoNoch keine Bewertungen
- Ribograma ProjectDokument59 SeitenRibograma Projectpirula123Noch keine Bewertungen
- In Their Own Words: Symptoms of Morgellons and Neuro-Cutaneous Syndrome (NCS)Dokument8 SeitenIn Their Own Words: Symptoms of Morgellons and Neuro-Cutaneous Syndrome (NCS)domasjeffersonNoch keine Bewertungen
- Classification of Lung Cancer - William Travis 2011Dokument9 SeitenClassification of Lung Cancer - William Travis 2011WeiLinNoch keine Bewertungen
- ACR Albumin Creatinine Ratio To Be PRESENTED BY HMN TO THE NEW MED TECH TRAINEES IN JAHRA HEALTH CENTER Apr 23 2014Dokument22 SeitenACR Albumin Creatinine Ratio To Be PRESENTED BY HMN TO THE NEW MED TECH TRAINEES IN JAHRA HEALTH CENTER Apr 23 2014honorinanuguidNoch keine Bewertungen
- Intravenous Injection of Coronavirus Disease 2019 (COVID-19) mRNA Vaccine Can Induce Acute Myopericarditis in Mouse ModelDokument18 SeitenIntravenous Injection of Coronavirus Disease 2019 (COVID-19) mRNA Vaccine Can Induce Acute Myopericarditis in Mouse ModelStacey KrellerNoch keine Bewertungen
- The Vaccine Adverse Event Reporting System (VAERS)Dokument356 SeitenThe Vaccine Adverse Event Reporting System (VAERS)Josh SingerNoch keine Bewertungen
- PLOTKINDokument6 SeitenPLOTKINElPaisUyNoch keine Bewertungen
- Redacted Paul Letter June 2014Dokument4 SeitenRedacted Paul Letter June 2014Heather X RhodesNoch keine Bewertungen
- SMCLK SJMC 09 2020 PDFDokument102 SeitenSMCLK SJMC 09 2020 PDFMarina JankovicNoch keine Bewertungen
- Ontario: Statement of Claim To The Defendant: A Legal Proceeding Has Been Commenced Against You by The PlaintiffsDokument49 SeitenOntario: Statement of Claim To The Defendant: A Legal Proceeding Has Been Commenced Against You by The PlaintiffsMagdolna Szalai PappNoch keine Bewertungen
- JURNALDokument12 SeitenJURNALAsMiraaaaNoch keine Bewertungen
- Platelet Transfusion: A Clinical Practice Guideline From The AABB FreeDokument6 SeitenPlatelet Transfusion: A Clinical Practice Guideline From The AABB FreeUJI MUTUNoch keine Bewertungen
- Rochwerg2020 Article TheRoleForHighFlowNasalCannulaDokument12 SeitenRochwerg2020 Article TheRoleForHighFlowNasalCannulaminiypuntoNoch keine Bewertungen
- Chapter 7. Pharmacokinetics of Oral AbsorptionDokument28 SeitenChapter 7. Pharmacokinetics of Oral AbsorptionbencleeseNoch keine Bewertungen
- Nwewsletter Spotlight Fall 2008Dokument16 SeitenNwewsletter Spotlight Fall 2008bencleeseNoch keine Bewertungen
- Chapter 1. Introduction To Medical ResearchDokument10 SeitenChapter 1. Introduction To Medical ResearchbencleeseNoch keine Bewertungen
- Harrison's Online ContentsDokument18 SeitenHarrison's Online Contentsbencleese0% (1)
- The TandemheartDokument6 SeitenThe TandemheartbencleeseNoch keine Bewertungen
- Basic & Clinical Biostatistics, 4th EditionDokument6 SeitenBasic & Clinical Biostatistics, 4th EditionbencleeseNoch keine Bewertungen
- INFLAMMATORY Breast CancerDokument20 SeitenINFLAMMATORY Breast CancerbencleeseNoch keine Bewertungen
- Lysosomal Disorders - PedsDokument38 SeitenLysosomal Disorders - PedsbencleeseNoch keine Bewertungen
- The Application of A Continuous Strip of Woven Material To A Body PartDokument15 SeitenThe Application of A Continuous Strip of Woven Material To A Body Partczeremar chanNoch keine Bewertungen
- HP-exampleDokument30 SeitenHP-exampleAnonymous 105zV1Noch keine Bewertungen
- Cross-Compilers: / / Running ARM Grub On U-Boot On QemuDokument5 SeitenCross-Compilers: / / Running ARM Grub On U-Boot On QemuSoukous LoverNoch keine Bewertungen
- BroucherDokument2 SeitenBroucherVishal PoulNoch keine Bewertungen
- MVC Plus User Manual REV5Dokument90 SeitenMVC Plus User Manual REV5Adalberto FentanezNoch keine Bewertungen
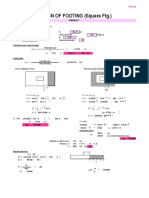
- Design of Footing (Square FTG.) : M Say, L 3.75Dokument2 SeitenDesign of Footing (Square FTG.) : M Say, L 3.75victoriaNoch keine Bewertungen
- Study On Color Fastness To Rubbing by Crock MeterDokument4 SeitenStudy On Color Fastness To Rubbing by Crock Metertushar100% (5)
- University of MauritiusDokument4 SeitenUniversity of MauritiusAtish KissoonNoch keine Bewertungen
- HAART PresentationDokument27 SeitenHAART PresentationNali peterNoch keine Bewertungen
- Midterm Quiz 1 March 9.2021 QDokument5 SeitenMidterm Quiz 1 March 9.2021 QThalia RodriguezNoch keine Bewertungen
- TrustworthinessDokument24 SeitenTrustworthinessJamsheed Raza100% (1)
- Exercises Service CostingDokument2 SeitenExercises Service Costingashikin dzulNoch keine Bewertungen
- Normas FieldbusDokument3 SeitenNormas FieldbusAlielson PazNoch keine Bewertungen
- Service Bulletin: Service Bulletin NUMBER: 8.8/134A Caterpillar: Confidential Green Page 1 of 8Dokument8 SeitenService Bulletin: Service Bulletin NUMBER: 8.8/134A Caterpillar: Confidential Green Page 1 of 8GutsavoNoch keine Bewertungen
- Business en Pre Above S+T ReadingDokument3 SeitenBusiness en Pre Above S+T Readingsvetlana939Noch keine Bewertungen
- Mannitol For Reduce IOPDokument7 SeitenMannitol For Reduce IOPHerryantoThomassawaNoch keine Bewertungen
- Gabuyer Oct13Dokument72 SeitenGabuyer Oct13William Rios0% (1)
- The Application of 1,2,3-PropanetriolDokument2 SeitenThe Application of 1,2,3-PropanetriolAlisameimeiNoch keine Bewertungen
- Ranking - Best Multivitamins in 2018Dokument7 SeitenRanking - Best Multivitamins in 2018JosephVillanuevaNoch keine Bewertungen
- Inteligen NT BB - NTC BB Datasheet PDFDokument4 SeitenInteligen NT BB - NTC BB Datasheet PDFfrancis erl ligsayNoch keine Bewertungen
- Gamesa Wind Turbine Element UpgradesDokument1 SeiteGamesa Wind Turbine Element Upgradesstanislav uzunchevNoch keine Bewertungen
- BCK Test Ans (Neha)Dokument3 SeitenBCK Test Ans (Neha)Neha GargNoch keine Bewertungen