Das könnte Ihnen auch gefallen
- Parthasarathy2013 PDFDokument7 SeitenParthasarathy2013 PDFAndi BintangNoch keine Bewertungen
- 1 s2.0 S0002937803001388 MainDokument3 Seiten1 s2.0 S0002937803001388 MainAndi BintangNoch keine Bewertungen
- Medical Hypotheses: Yixian Li, Juan Zhou, Ian Burkovskiy, Pollen Yeung, Christian Lehmann TDokument3 SeitenMedical Hypotheses: Yixian Li, Juan Zhou, Ian Burkovskiy, Pollen Yeung, Christian Lehmann TAndi BintangNoch keine Bewertungen
- Subarachnoid Block For Caesarean Section in Severe PreeclampsiaDokument6 SeitenSubarachnoid Block For Caesarean Section in Severe PreeclampsiaAndi BintangNoch keine Bewertungen
- 1 s2.0 S0002937803001388 MainDokument3 Seiten1 s2.0 S0002937803001388 MainAndi BintangNoch keine Bewertungen
- Depresión e InmunidadDokument13 SeitenDepresión e InmunidadgabisaenaNoch keine Bewertungen
- Bar A Zanchi 2018Dokument17 SeitenBar A Zanchi 2018Andi BintangNoch keine Bewertungen
- Anestesia General para Césarea PDFDokument7 SeitenAnestesia General para Césarea PDFAgnese ValentiniNoch keine Bewertungen
- Anestesia General para Césarea PDFDokument7 SeitenAnestesia General para Césarea PDFAgnese ValentiniNoch keine Bewertungen
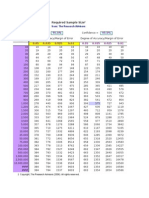
- Required Sample Size: From: The Research AdvisorsDokument3 SeitenRequired Sample Size: From: The Research AdvisorsAbhishek Sharma100% (1)
- Procalcitonin As A Biomarker of Severity Degree in Sepsis Due To PneumoniaDokument5 SeitenProcalcitonin As A Biomarker of Severity Degree in Sepsis Due To PneumoniaAndi BintangNoch keine Bewertungen
- 1 s2.0 S0002937800704534 Main PDFDokument1 Seite1 s2.0 S0002937800704534 Main PDFAndi BintangNoch keine Bewertungen
- Cultural Sociology of Mental Illness n28Dokument5 SeitenCultural Sociology of Mental Illness n28Andi BintangNoch keine Bewertungen
- Overweight linked to increased risk of lower back painDokument8 SeitenOverweight linked to increased risk of lower back painAndi BintangNoch keine Bewertungen
- Instruction For Author ClimactericDokument9 SeitenInstruction For Author ClimactericAndi BintangNoch keine Bewertungen
- 1 s2.0 S1052305714000561 MainDokument6 Seiten1 s2.0 S1052305714000561 MainAndi BintangNoch keine Bewertungen
- Hepatitis C APASLfghDokument27 SeitenHepatitis C APASLfghAndi BintangNoch keine Bewertungen
- Sacral Nerve Stimulation Reduces Elevated Urinary Nerve Growth Factor Levels in Women With Symptomatic Detrusor OveractivityDokument5 SeitenSacral Nerve Stimulation Reduces Elevated Urinary Nerve Growth Factor Levels in Women With Symptomatic Detrusor OveractivityAndi BintangNoch keine Bewertungen
- 1 s2.0 S0021755713002003 MainDokument6 Seiten1 s2.0 S0021755713002003 MainAndi BintangNoch keine Bewertungen
- 1 s2.0 S0021755713002003 MainDokument6 Seiten1 s2.0 S0021755713002003 MainAndi BintangNoch keine Bewertungen
- Association Between Constipation and Colorectal Cancer Systematic Review and Meta-Analysis of Observational StusdgdiesDokument10 SeitenAssociation Between Constipation and Colorectal Cancer Systematic Review and Meta-Analysis of Observational StusdgdiesAndi BintangNoch keine Bewertungen
- 2013 Student Membership ApplicationDokument1 Seite2013 Student Membership ApplicationAndi BintangNoch keine Bewertungen
- Prevalence of Diabetes and Impaired Fasting Glucose in Adults in The U.S. PopulationDokument6 SeitenPrevalence of Diabetes and Impaired Fasting Glucose in Adults in The U.S. PopulationAndi BintangNoch keine Bewertungen
- Anthropometry: Ergonomics Additional ResourcesDokument5 SeitenAnthropometry: Ergonomics Additional ResourcesAndi BintangNoch keine Bewertungen
- Serviks DocjhjuDokument366 SeitenServiks DocjhjuAndi BintangNoch keine Bewertungen
- Urologi PDFDokument237 SeitenUrologi PDFAndi BintangNoch keine Bewertungen
- MK Giz Slide Infant Feeding PracticeDokument1 SeiteMK Giz Slide Infant Feeding PracticeAndi BintangNoch keine Bewertungen
- ATS Guidelines CAP ManagementDokument25 SeitenATS Guidelines CAP ManagementMae Matira AbeladorNoch keine Bewertungen
- PCT CAP ABiuytoDokument10 SeitenPCT CAP ABiuytoAndi BintangNoch keine Bewertungen
- Cap Bts 2009 ComplitdgDokument139 SeitenCap Bts 2009 ComplitdgAndi BintangNoch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Shraddha ProjectDokument8 SeitenShraddha ProjectshraddhagandhiNoch keine Bewertungen
- Benalcazar-Parra 2019 Physiol. Meas. 40 085003Dokument13 SeitenBenalcazar-Parra 2019 Physiol. Meas. 40 085003Carlos Antonio BenalcazarNoch keine Bewertungen
- Transecting Versus Avoiding Incision of The Anterior PlacentaDokument23 SeitenTransecting Versus Avoiding Incision of The Anterior PlacentaRirinNoch keine Bewertungen
- Journal ReadingDokument13 SeitenJournal ReadingFahrika Luthfi AfiqohNoch keine Bewertungen
- CoparDokument51 SeitenCoparGregg PalabricaNoch keine Bewertungen
- Ethics Alaa MCQs and Notes - 1Dokument21 SeitenEthics Alaa MCQs and Notes - 1maimoona suleman100% (1)
- MCQs and Best Answer. (١)Dokument19 SeitenMCQs and Best Answer. (١)Rehab KhiderNoch keine Bewertungen
- Proforma For Registration of Subject For DissertationDokument33 SeitenProforma For Registration of Subject For DissertationRaafi Puristya Aries DarmawanNoch keine Bewertungen
- Rajeev Kumar Talakayala CVDokument37 SeitenRajeev Kumar Talakayala CVSanjeev KumarNoch keine Bewertungen
- Birth Canal Injuries Final LectureDokument63 SeitenBirth Canal Injuries Final Lecturepeter njoguNoch keine Bewertungen
- PRC FORM 106 RECORD OF ACTUAL DELIVERIESDokument4 SeitenPRC FORM 106 RECORD OF ACTUAL DELIVERIESmaricel dogweNoch keine Bewertungen
- Dri Na Hi Noveline TanDokument1 SeiteDri Na Hi Noveline TanZachary BañezNoch keine Bewertungen
- Wellness Centre AccreditationDokument112 SeitenWellness Centre AccreditationAA TNoch keine Bewertungen
- Abnormal Uterine Action GuideDokument27 SeitenAbnormal Uterine Action Guidetanmai noolu100% (1)
- The Implications of Shortages of Health Professionals For Maternal Health in Sub Saharan AfricaDokument12 SeitenThe Implications of Shortages of Health Professionals For Maternal Health in Sub Saharan AfricaBilal AhmadNoch keine Bewertungen
- WWW Drshraddhagalgali Com Pregnancy CareDokument2 SeitenWWW Drshraddhagalgali Com Pregnancy CareShraddha GalgaliNoch keine Bewertungen
- Contracted Pelvis: Rupture of The UterusDokument42 SeitenContracted Pelvis: Rupture of The UterusMed PoxNoch keine Bewertungen
- Uprak Rubrik Bu IzfaaizahDokument12 SeitenUprak Rubrik Bu IzfaaizahMaya Ulfah apriliyaNoch keine Bewertungen
- ATI Maternal Newborn Chapter 1-ContraceptionDokument23 SeitenATI Maternal Newborn Chapter 1-ContraceptionVin Lorenzo Campbell100% (4)
- Einc Skills ChecklistDokument3 SeitenEinc Skills ChecklistKENT AUSTRIANoch keine Bewertungen
- Telenursing Jurnal Stress in Mother PDFDokument7 SeitenTelenursing Jurnal Stress in Mother PDFNaniNoch keine Bewertungen
- IRDSDokument17 SeitenIRDSJustin Ahorro-DionisioNoch keine Bewertungen
- Edit Lagi JOURNAL READING AND CRITICAL APPRAISAL SONOGRAPHIC CLDokument25 SeitenEdit Lagi JOURNAL READING AND CRITICAL APPRAISAL SONOGRAPHIC CLvina zulfianiNoch keine Bewertungen
- Maternal and Child Nursing Topic Exam 1Dokument4 SeitenMaternal and Child Nursing Topic Exam 1james_manuel111870840% (1)
- Maternal and Child Health NursingDokument17 SeitenMaternal and Child Health NursingSarah Jane MaganteNoch keine Bewertungen
- 1Dokument138 Seiten1Yasser Ahmed0% (1)
- Nfhs-5 India ReportDokument713 SeitenNfhs-5 India ReportROHIT DASNoch keine Bewertungen
- Sri Ramachandra University Nursing SyllabusDokument9 SeitenSri Ramachandra University Nursing SyllabusEric ReubenNoch keine Bewertungen
- High Yield Obs & GynaeDokument84 SeitenHigh Yield Obs & GynaeDrive RashNoch keine Bewertungen
- Immediate Newborn CareDokument3 SeitenImmediate Newborn CareAlyssa Malsi NacinoNoch keine Bewertungen