Das könnte Ihnen auch gefallen
- 17 Ways To Beat Erectile DysfunctionDokument21 Seiten17 Ways To Beat Erectile Dysfunctionrlscott50% (2)
- DD Palmer Chronology PDFDokument42 SeitenDD Palmer Chronology PDFAdam BrowningNoch keine Bewertungen
- Dizziness - Vertigo and HomoeopathyDokument38 SeitenDizziness - Vertigo and HomoeopathyDr. Rajneesh Kumar Sharma MD HomNoch keine Bewertungen
- Strawberry Dna Extract KitDokument18 SeitenStrawberry Dna Extract KitIcunLelah Hatilelah SekaliampebngungdirisndriNoch keine Bewertungen
- Urine The Spotlight. Urine Therapy Newsletter Debut - by Urine The Spotlight - Nov, 2021 - MediumDokument28 SeitenUrine The Spotlight. Urine Therapy Newsletter Debut - by Urine The Spotlight - Nov, 2021 - Mediuminfo-501699Noch keine Bewertungen
- Abp Dynamics Multiple Choice 2016-02-24Dokument10 SeitenAbp Dynamics Multiple Choice 2016-02-24artsidartsyNoch keine Bewertungen
- Nerve CellDokument45 SeitenNerve Cellapi-420631518Noch keine Bewertungen
- MeiosisDokument39 SeitenMeiosisوجدان الشداديNoch keine Bewertungen
- EMBRYONIC STEM CELLS AND HUMAN LIFEDokument11 SeitenEMBRYONIC STEM CELLS AND HUMAN LIFEGeorge AtaherNoch keine Bewertungen
- STATICSDokument33 SeitenSTATICSRandy NatalNoch keine Bewertungen
- Qualitative Analysis 2Dokument81 SeitenQualitative Analysis 2nateq oikNoch keine Bewertungen
- 1 - The Origin and Systems of EarthDokument54 Seiten1 - The Origin and Systems of EarthFran SethNoch keine Bewertungen
- Tumor marker classification and applicationsDokument30 SeitenTumor marker classification and applicationsnouval_iqbal100% (1)
- Tumor marker classification and applicationsDokument30 SeitenTumor marker classification and applicationsnouval_iqbal100% (1)
- Paediatric History Collection FormatDokument7 SeitenPaediatric History Collection FormatSathya Palanisamy100% (1)
- Essentials of Diagnosis and Treatment of Acute LeukemiaDokument16 SeitenEssentials of Diagnosis and Treatment of Acute Leukemianouval_iqbalNoch keine Bewertungen
- Sesq PDFDokument11 SeitenSesq PDFClint CamNoch keine Bewertungen
- Practice Quiz For EpidemiologyDokument4 SeitenPractice Quiz For EpidemiologyOsama Alhumisi100% (3)
- Exercise The MicroscopeDokument15 SeitenExercise The Microscopemydiamondstar17Noch keine Bewertungen
- Retraction Ring LeafletDokument2 SeitenRetraction Ring LeafletAna100% (1)
- Olimpiada Engleza 2017 CL A 8A PDFDokument4 SeitenOlimpiada Engleza 2017 CL A 8A PDFAnthony AdamsNoch keine Bewertungen
- Evolution - How Species ChangeDokument29 SeitenEvolution - How Species ChangeGhaash BabaNoch keine Bewertungen
- Characteristics of LifeDokument5 SeitenCharacteristics of LifeVan Denver E. BautistaNoch keine Bewertungen
- The Home of The AshfallDokument3 SeitenThe Home of The AshfallJoemel Mark Mamugay50% (2)
- Assessing Public Terminal Operations in Lapu-Lapu CityDokument10 SeitenAssessing Public Terminal Operations in Lapu-Lapu CityCris Paolo RafolsNoch keine Bewertungen
- Computer EssentialsDokument28 SeitenComputer EssentialsJeiyo Dela CruzNoch keine Bewertungen
- Unity Amidst DiversityDokument23 SeitenUnity Amidst DiversityhezekiahNoch keine Bewertungen
- Lab02 Experiment1Dokument4 SeitenLab02 Experiment1Mike86% (7)
- Components of System UnitDokument11 SeitenComponents of System UnitAli ZeeshanNoch keine Bewertungen
- Ethics Position PaperDokument8 SeitenEthics Position Papercwise2100% (1)
- Turner SyndromeDokument2 SeitenTurner SyndromeStephen YapNoch keine Bewertungen
- 2 - Evolution NotesDokument38 Seiten2 - Evolution Notesapi-375285021Noch keine Bewertungen
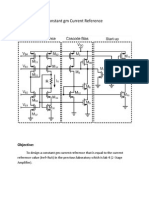
- Constant GM Current ReferenceDokument4 SeitenConstant GM Current ReferenceGp GonzalesNoch keine Bewertungen
- Anatomy of Computer SystemDokument9 SeitenAnatomy of Computer Systemfaraz100% (1)
- Plant Physiology Course HandoutDokument3 SeitenPlant Physiology Course HandoutAryaman MandhanaNoch keine Bewertungen
- Chromosome Abnormalities and Sex DeterminationDokument43 SeitenChromosome Abnormalities and Sex DeterminationprasadbheemNoch keine Bewertungen
- 7 Characteristics of LifeDokument10 Seiten7 Characteristics of LifeSarah RobertNoch keine Bewertungen
- MSc Microbiology Syllabus Bharathidasan UniversityDokument28 SeitenMSc Microbiology Syllabus Bharathidasan UniversitysertysdhuaosdjiNoch keine Bewertungen
- Cystic FibrosisDokument3 SeitenCystic FibrosissakthiprimeNoch keine Bewertungen
- DNA Extraction LabDokument3 SeitenDNA Extraction Labalexander justin tanhuecoNoch keine Bewertungen
- France Grading SystemDokument6 SeitenFrance Grading SystemClara AlbertNoch keine Bewertungen
- Genetics) SyllabusDokument33 SeitenGenetics) Syllabusb.duttaNoch keine Bewertungen
- Protein Chemistry Section ExamDokument9 SeitenProtein Chemistry Section ExamJoelNoch keine Bewertungen
- Lab Report RubricsDokument4 SeitenLab Report Rubricsapi-270861823Noch keine Bewertungen
- Biochem COURSE SYLLABUSDokument10 SeitenBiochem COURSE SYLLABUSSharmaine DurangoNoch keine Bewertungen
- Learn Your StyleDokument7 SeitenLearn Your StyleSulaymaanNoch keine Bewertungen
- Assignment On EarthquakeDokument14 SeitenAssignment On EarthquakeAkash Sahu100% (2)
- Genetics Lesson PlanDokument4 SeitenGenetics Lesson Plankayla08Noch keine Bewertungen
- DLL - Trigo 7Dokument2 SeitenDLL - Trigo 7Gel KilalaNoch keine Bewertungen
- Effect of Salinity On Seed Germination, Growth and Organic Compounds of Mungbean Plant Vigna RadiataDokument10 SeitenEffect of Salinity On Seed Germination, Growth and Organic Compounds of Mungbean Plant Vigna RadiatahunarsandhuNoch keine Bewertungen
- The Mesozoic and Cenozoic EraDokument28 SeitenThe Mesozoic and Cenozoic EraLuca LK100% (1)
- Revised Paperworks of Group 2, IV - GalileoDokument42 SeitenRevised Paperworks of Group 2, IV - GalileoAgatha Dominique Bacani0% (2)
- The Theory of EvolutionDokument9 SeitenThe Theory of EvolutionElana SokalNoch keine Bewertungen
- Biochemistry: NTA Level 6 Facilitator's Guide For Diploma in NursingDokument68 SeitenBiochemistry: NTA Level 6 Facilitator's Guide For Diploma in NursingEmanuel Acray NkondolaNoch keine Bewertungen
- Neem Biodiesel by BashasDokument60 SeitenNeem Biodiesel by BashasmohideenbashaNoch keine Bewertungen
- Purposive SamplingDokument1 SeitePurposive SamplingMichelle Romasoc CasipitNoch keine Bewertungen
- Characteristics of Sound WavesDokument15 SeitenCharacteristics of Sound WavesBlessy Martin100% (1)
- Active vs Passive Voice GuideDokument8 SeitenActive vs Passive Voice GuideccaanlNoch keine Bewertungen
- Genetically Modified OrganismsDokument3 SeitenGenetically Modified OrganismsSandip ThapaNoch keine Bewertungen
- Activity 1Dokument5 SeitenActivity 1dave bryan manguilimotan100% (1)
- Scientific Method For DummiesDokument4 SeitenScientific Method For DummiesBill KolesnikNoch keine Bewertungen
- Seed Germination FactorsDokument17 SeitenSeed Germination FactorsDelos Santos JosephNoch keine Bewertungen
- 2 TestosteroneDokument20 Seiten2 TestosteroneZiedTrikiNoch keine Bewertungen
- Creative writing exam preparationDokument15 SeitenCreative writing exam preparationgrazielarepuyoNoch keine Bewertungen
- How to Build a Strong PositionDokument11 SeitenHow to Build a Strong PositioniK ONNoch keine Bewertungen
- Evolution 101Dokument102 SeitenEvolution 101IWantToBelieve8728100% (2)
- Protein Synthesis Transcription and Translation Distance LearningDokument10 SeitenProtein Synthesis Transcription and Translation Distance LearningjaneyzhouNoch keine Bewertungen
- HL IB Biology II - Seed Germination LabDokument4 SeitenHL IB Biology II - Seed Germination LabtyrekethomasNoch keine Bewertungen
- Art CubismDokument23 SeitenArt CubismBraiyle ENoch keine Bewertungen
- S7. Turner SyndromeDokument5 SeitenS7. Turner SyndromeAxSlzrNoch keine Bewertungen
- Paedia - Dr. RehabDokument173 SeitenPaedia - Dr. RehabMohammed Saad NabhanNoch keine Bewertungen
- Pelvic PainDokument2 SeitenPelvic Painnouval_iqbalNoch keine Bewertungen
- Microtherm Heat Stress WBGT Competitor TableDokument1 SeiteMicrotherm Heat Stress WBGT Competitor Tablenouval_iqbalNoch keine Bewertungen
- Drug Dose IqbalDokument2 SeitenDrug Dose Iqbalnouval_iqbalNoch keine Bewertungen
- Daftar PustakaDokument1 SeiteDaftar Pustakanouval_iqbalNoch keine Bewertungen
- Pathophysiology of Postpartum Hemorrhage and Third Stage of LaborDokument7 SeitenPathophysiology of Postpartum Hemorrhage and Third Stage of Labornouval_iqbalNoch keine Bewertungen
- Lab Results SummaryDokument1 SeiteLab Results Summarynouval_iqbalNoch keine Bewertungen
- Drug Dose 2Dokument3 SeitenDrug Dose 2nouval_iqbalNoch keine Bewertungen
- B6 Hole FormDokument1 SeiteB6 Hole Formnouval_iqbalNoch keine Bewertungen
- Bed: Identitas: MRS: Diagnosis: DR.: TGL Subjective & Objective Lab/Radiology Assessment & PlanningDokument3 SeitenBed: Identitas: MRS: Diagnosis: DR.: TGL Subjective & Objective Lab/Radiology Assessment & Planningnouval_iqbalNoch keine Bewertungen
- Pain ManagementDokument37 SeitenPain Managementnouval_iqbalNoch keine Bewertungen
- Bed: Identitas: MRS: Diagnosis: DR.: TGL Subjective & Objective Lab/Radiology Assessment & PlanningDokument3 SeitenBed: Identitas: MRS: Diagnosis: DR.: TGL Subjective & Objective Lab/Radiology Assessment & Planningnouval_iqbalNoch keine Bewertungen
- Coagulation 2006 A Modern View of HemostasisDokument11 SeitenCoagulation 2006 A Modern View of HemostasisCarlos AlfaroNoch keine Bewertungen
- Hari 1 Sayap +bisep Hari2 Bahu + Kaki Hari 3 Dada + Trisep Hari 4 Sayap + Bisep Hari 5 Bahu + Kaki Hari 6 Dada + TrisepsDokument1 SeiteHari 1 Sayap +bisep Hari2 Bahu + Kaki Hari 3 Dada + Trisep Hari 4 Sayap + Bisep Hari 5 Bahu + Kaki Hari 6 Dada + Trisepsnouval_iqbalNoch keine Bewertungen
- Lab Results SummaryDokument1 SeiteLab Results Summarynouval_iqbalNoch keine Bewertungen
- Understanding The Symptoms of The Common Cold and Influenza PDFDokument8 SeitenUnderstanding The Symptoms of The Common Cold and Influenza PDFnouval_iqbalNoch keine Bewertungen
- Methods For Assessing Leg Length DiscrepancyDokument13 SeitenMethods For Assessing Leg Length DiscrepancyKanika SinhaNoch keine Bewertungen
- Protein intake and atherosclerosisDokument7 SeitenProtein intake and atherosclerosisnouval_iqbalNoch keine Bewertungen
- MAKE IT MINE - Wake Up and Seize Your DreamsDokument1 SeiteMAKE IT MINE - Wake Up and Seize Your Dreamsnouval_iqbalNoch keine Bewertungen
- Thesis PDFDokument20 SeitenThesis PDFnouval_iqbalNoch keine Bewertungen
- Red Meat Consumption An Overview of The Risks and Benefits PDFDokument13 SeitenRed Meat Consumption An Overview of The Risks and Benefits PDFnouval_iqbalNoch keine Bewertungen
- PR DR YanceDokument5 SeitenPR DR Yancenouval_iqbalNoch keine Bewertungen
- 3426 4774 1 SMDokument6 Seiten3426 4774 1 SMnouval_iqbalNoch keine Bewertungen
- Dubowitz ScoreDokument3 SeitenDubowitz ScorentadudulNoch keine Bewertungen
- Pelvic PainDokument2 SeitenPelvic Painnouval_iqbalNoch keine Bewertungen
- Tumor Tractus UrogenitalDokument17 SeitenTumor Tractus Urogenitalnouval_iqbalNoch keine Bewertungen
- Low Levels of Fibrin-Stabilizing Factor (Factor Xiii) in Human Plasmodium Falciparum Malaria Correlation With Clinical Severity PDFDokument6 SeitenLow Levels of Fibrin-Stabilizing Factor (Factor Xiii) in Human Plasmodium Falciparum Malaria Correlation With Clinical Severity PDFnouval_iqbalNoch keine Bewertungen
- Changes in The Total Leukocyte and Platelet Counts in Papuan and Non Papuan Adults From Northeast Papua PDFDokument8 SeitenChanges in The Total Leukocyte and Platelet Counts in Papuan and Non Papuan Adults From Northeast Papua PDFnouval_iqbalNoch keine Bewertungen
- What Is African Trypanosomiasis?Dokument3 SeitenWhat Is African Trypanosomiasis?dean016026Noch keine Bewertungen
- Drugs of Choice - CompiledDokument18 SeitenDrugs of Choice - CompiledAvinash DesaiNoch keine Bewertungen
- Internship Presentation ServalishsDokument15 SeitenInternship Presentation Servalishsapi-334247133Noch keine Bewertungen
- Marijuana and EpilepsyDokument17 SeitenMarijuana and EpilepsyOmar AntabliNoch keine Bewertungen
- Nurs Fpx 4050 Assessment 1 Preliminary Care Coordination PlanDokument4 SeitenNurs Fpx 4050 Assessment 1 Preliminary Care Coordination Planfarwaamjad771Noch keine Bewertungen
- Patient Scenario, Chapter 19, Nutritional Needs of A NewbornDokument3 SeitenPatient Scenario, Chapter 19, Nutritional Needs of A NewbornNobiliary ortizNoch keine Bewertungen
- Writing OETDokument4 SeitenWriting OETfernanda1rondelliNoch keine Bewertungen
- Mental Status Examination - StatPearls - NCBI BookshelfDokument9 SeitenMental Status Examination - StatPearls - NCBI BookshelfGRUPO DE INTERES EN PSIQUIATRIANoch keine Bewertungen
- Managed Care, Hospitals' Hit Tolerable When Covid Emergency EndsDokument5 SeitenManaged Care, Hospitals' Hit Tolerable When Covid Emergency EndsCarlos Mendoza DomínguezNoch keine Bewertungen
- Diabetes in Pregnancy: Management ofDokument8 SeitenDiabetes in Pregnancy: Management ofdiana rossNoch keine Bewertungen
- GERD DR Hegar Dec2015Dokument52 SeitenGERD DR Hegar Dec2015nur_betaNoch keine Bewertungen
- Reading Sample Test 1 Question Paper Part A PDFDokument4 SeitenReading Sample Test 1 Question Paper Part A PDFnavroop bajwaNoch keine Bewertungen
- Fansidar Drug StudyDokument2 SeitenFansidar Drug StudyjangzieNoch keine Bewertungen
- (14374331 - Clinical Chemistry and Laboratory Medicine (CCLM) ) Measurement Uncertainty - Light in The ShadowsDokument3 Seiten(14374331 - Clinical Chemistry and Laboratory Medicine (CCLM) ) Measurement Uncertainty - Light in The ShadowsJulián Mesa SierraNoch keine Bewertungen
- Shalya Paper-I PDFDokument17 SeitenShalya Paper-I PDFSusmita VinupamulaNoch keine Bewertungen
- SAGO Pharma Inc Rev2.1Dokument17 SeitenSAGO Pharma Inc Rev2.1wafaa mustafaNoch keine Bewertungen
- Medical Leave CertificatesDokument4 SeitenMedical Leave CertificatesDhana LakshmiNoch keine Bewertungen
- Hope 11 Assessment 1 4TH QTRDokument2 SeitenHope 11 Assessment 1 4TH QTRApril Rose Ferrancullo RelojNoch keine Bewertungen
- Ultrasound Findings in FIP CatsDokument73 SeitenUltrasound Findings in FIP Catsludiegues752Noch keine Bewertungen
- Bupivacaine (Marcaine)Dokument2 SeitenBupivacaine (Marcaine)Michalis SpyridakisNoch keine Bewertungen
- CHF SIM - Preparation Questions and Notes For LPN StudentsDokument3 SeitenCHF SIM - Preparation Questions and Notes For LPN Studentsmercy longNoch keine Bewertungen