Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Marc Lobliner - Fat Loss Factor BookDokument77 SeitenMarc Lobliner - Fat Loss Factor Bookcleudimartins100% (2)
- AP Economy in BriefDokument77 SeitenAP Economy in Briefdarimadugu100% (1)
- A Nutty Way To Measure CaloriesDokument2 SeitenA Nutty Way To Measure CaloriesDavid PhamNoch keine Bewertungen
- Copper Kettle Catering 2Dokument4 SeitenCopper Kettle Catering 2t4thilini100% (2)
- Ultimate Guide To Marathon Running 2nd Edition PDFDokument164 SeitenUltimate Guide To Marathon Running 2nd Edition PDFJordi LopezNoch keine Bewertungen
- Aspartame 2012 Final PDFDokument10 SeitenAspartame 2012 Final PDFdocneiraNoch keine Bewertungen
- Thimerosal y ASDDokument12 SeitenThimerosal y ASDdocneiraNoch keine Bewertungen
- Asian Pac. J. Allergy Immunol. 2013 Amarasekera PDFDokument10 SeitenAsian Pac. J. Allergy Immunol. 2013 Amarasekera PDFdocneiraNoch keine Bewertungen
- Respiracion y Control Metabolico y Oxidativo PDFDokument3 SeitenRespiracion y Control Metabolico y Oxidativo PDFdocneiraNoch keine Bewertungen
- Aspartamo y Obesidad PDFDokument7 SeitenAspartamo y Obesidad PDFdocneiraNoch keine Bewertungen
- Carne Roja y MortalidadDokument9 SeitenCarne Roja y MortalidaddocneiraNoch keine Bewertungen
- Chinese Herbal Mixture y Cancer PDFDokument7 SeitenChinese Herbal Mixture y Cancer PDFdocneiraNoch keine Bewertungen
- Ajo y Neumonía Por Bacteria Multiresistente PDFDokument2 SeitenAjo y Neumonía Por Bacteria Multiresistente PDFdocneiraNoch keine Bewertungen
- Ajo y Efecto Antibiótico PDFDokument6 SeitenAjo y Efecto Antibiótico PDFdocneiraNoch keine Bewertungen
- Cerebro y Meditacion PDFDokument18 SeitenCerebro y Meditacion PDFdocneiraNoch keine Bewertungen
- Meditacion y RM Cerebral PDFDokument7 SeitenMeditacion y RM Cerebral PDFdocneiraNoch keine Bewertungen
- Isoflavonas y Cancer de Prostata PDFDokument4 SeitenIsoflavonas y Cancer de Prostata PDFdocneiraNoch keine Bewertungen
- Meditacion y Autismo PDFDokument11 SeitenMeditacion y Autismo PDFdocneiraNoch keine Bewertungen
- Autismo y Vacunacion PDFDokument15 SeitenAutismo y Vacunacion PDFdocneiraNoch keine Bewertungen
- Cancer Otto Warburg 00Dokument7 SeitenCancer Otto Warburg 00Harish BorraNoch keine Bewertungen
- Vacuna Hepatitis B y Autismo PDFDokument14 SeitenVacuna Hepatitis B y Autismo PDFdocneiraNoch keine Bewertungen
- The Toxic Truth About SugarDokument3 SeitenThe Toxic Truth About SugarfatoldfartNoch keine Bewertungen
- SBS Instalment Plans at 0% Markup : Alfalah Credit CardsDokument2 SeitenSBS Instalment Plans at 0% Markup : Alfalah Credit CardsSyeda SeeratNoch keine Bewertungen
- English 4 Q4 Week 1Dokument82 SeitenEnglish 4 Q4 Week 1Pia PrenroseNoch keine Bewertungen
- 历年托福词汇题汇总440题Dokument54 Seiten历年托福词汇题汇总440题harry yangNoch keine Bewertungen
- IELTS Practice TestDokument4 SeitenIELTS Practice TestDániel KreiszNoch keine Bewertungen
- Eyesight Self Correction Instructions 2Dokument19 SeitenEyesight Self Correction Instructions 2Brad YantzerNoch keine Bewertungen
- Dietary Intake, Nutrient Status, and Growth Parameters in Children With Autism SpectrumDokument8 SeitenDietary Intake, Nutrient Status, and Growth Parameters in Children With Autism Spectrumguilherme augusto paroNoch keine Bewertungen
- Rewrite The Following Sentences Into Active VoiceDokument2 SeitenRewrite The Following Sentences Into Active VoiceTamara GonzalezNoch keine Bewertungen
- Lincoln County School District # 2 Elementary Lunch Menu January-11Dokument1 SeiteLincoln County School District # 2 Elementary Lunch Menu January-11anon-579447Noch keine Bewertungen
- Jack-Large Mouth BassDokument2 SeitenJack-Large Mouth Basslbrinson1Noch keine Bewertungen
- Fun Butterfly SnacksDokument5 SeitenFun Butterfly Snacksapi-637009748Noch keine Bewertungen
- Final Exam in PE and Health 10Dokument1 SeiteFinal Exam in PE and Health 10Mary Grace Palis-MaulionNoch keine Bewertungen
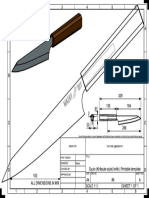
- 06 Gyuto Knife DRWDokument1 Seite06 Gyuto Knife DRWPeter IlievNoch keine Bewertungen
- Birthday Celeb Madam MarlynDokument3 SeitenBirthday Celeb Madam MarlynEric PascuaNoch keine Bewertungen
- In Partial FulfillmentDokument17 SeitenIn Partial FulfillmentHarvey Jansen JrNoch keine Bewertungen
- Level Test EnglishDokument6 SeitenLevel Test EnglishCelia Romero MateoNoch keine Bewertungen
- Gastronomic Tourism, A New Trend For Contemporary Tourism??: Georgică Gheorghe, Petronela Tudorache, Puiu NistoreanuDokument10 SeitenGastronomic Tourism, A New Trend For Contemporary Tourism??: Georgică Gheorghe, Petronela Tudorache, Puiu NistoreanuMuhammad RojaliNoch keine Bewertungen
- IFRJ 2017, Sri Winarti, Colonic MicrobiotaDokument8 SeitenIFRJ 2017, Sri Winarti, Colonic MicrobiotaSri WinartiNoch keine Bewertungen
- Pengaruh Sp-36 Dan Asam Humat Terhadap Pertumbuhan Dan Produksi Tanaman Kedelai (Glycine Max L)Dokument6 SeitenPengaruh Sp-36 Dan Asam Humat Terhadap Pertumbuhan Dan Produksi Tanaman Kedelai (Glycine Max L)Alif FazariNoch keine Bewertungen
- Differences Between Trends and FadsDokument19 SeitenDifferences Between Trends and FadsRhea Carillo100% (3)
- Natural Glow BookDokument112 SeitenNatural Glow Bookalejandra9roper9cond100% (1)
- Let's Be HealthyDokument4 SeitenLet's Be HealthygizlealvesNoch keine Bewertungen
- A Restaurant Review and RubricDokument2 SeitenA Restaurant Review and Rubricandres aponteNoch keine Bewertungen
- Flexible Dieting 1Dokument11 SeitenFlexible Dieting 1SamirNoch keine Bewertungen
- NG T Đi V I Gi I T - Phrasal VerbsDokument13 SeitenNG T Đi V I Gi I T - Phrasal VerbsĐỗ Thị Hồng NguyênNoch keine Bewertungen
- The Triumph of Surgery Notes Class 10 NCERT EnglishDokument4 SeitenThe Triumph of Surgery Notes Class 10 NCERT EnglishRudar SharmaNoch keine Bewertungen
- Semester I Lesson 1 FamilyDokument60 SeitenSemester I Lesson 1 FamilyPuspita Purnama SariNoch keine Bewertungen