Das könnte Ihnen auch gefallen
- Postpartum Depression: Clinical PracticeDokument11 SeitenPostpartum Depression: Clinical PracticeCasey Daisiu100% (1)
- Sailing To ByzantiumDokument23 SeitenSailing To ByzantiumVictor Hugo Esquivel0% (1)
- Maternity - Postnatal Care in The First Week - CG - 2015Dokument41 SeitenMaternity - Postnatal Care in The First Week - CG - 2015Monica SurduNoch keine Bewertungen
- Postpartum PsychosisDokument25 SeitenPostpartum PsychosisWinset Bimbitz JacotNoch keine Bewertungen
- Treatment and Management of Mental Health Conditions During Pregnancy and Postpartum ACOG June 2023Dokument27 SeitenTreatment and Management of Mental Health Conditions During Pregnancy and Postpartum ACOG June 2023kaiorm2k100% (3)
- Grabar Andre The Art of The Byzantine Empire 1967Dokument234 SeitenGrabar Andre The Art of The Byzantine Empire 1967sorin2013100% (19)
- Standards of Psychiatric Mental Health NursingDokument33 SeitenStandards of Psychiatric Mental Health NursingSANU RAMASWAMY100% (1)
- Manila Health Department ProgramsDokument5 SeitenManila Health Department Programsana dizonNoch keine Bewertungen
- Postpartum NCPDokument20 SeitenPostpartum NCPapi-370148988% (34)
- Persian Occupation of Egypt 619 6291Dokument16 SeitenPersian Occupation of Egypt 619 6291Victor Hugo EsquivelNoch keine Bewertungen
- Byzantium and BulgariaDokument28 SeitenByzantium and BulgariaVictor Hugo EsquivelNoch keine Bewertungen
- Mental Illness BrochureDokument24 SeitenMental Illness BrochureRyanna A SempleNoch keine Bewertungen
- Nur 2310 Maternal Exam Questions and AnswersDokument80 SeitenNur 2310 Maternal Exam Questions and AnswersNelson MandelaNoch keine Bewertungen
- Dark Age WarriorDokument140 SeitenDark Age WarriorVictor Hugo Esquivel100% (3)
- Byzantine ArchitectureDokument22 SeitenByzantine ArchitectureVictor Hugo EsquivelNoch keine Bewertungen
- Key Answers On The ExamDokument81 SeitenKey Answers On The ExamKarl Kiw-isNoch keine Bewertungen
- Postnatal Assessment FormatDokument16 SeitenPostnatal Assessment FormatValarmathi92% (13)
- A Checklist of Bishops in Byzantine Egypt PDFDokument38 SeitenA Checklist of Bishops in Byzantine Egypt PDFVictor Hugo EsquivelNoch keine Bewertungen
- Prevalence of Depression Among Saudi Pregnant WomenDokument8 SeitenPrevalence of Depression Among Saudi Pregnant WomenIOSRjournalNoch keine Bewertungen
- Byzantium 039 S Balkan Frontier A Political Study of The Northern Balkans 900 1204Dokument366 SeitenByzantium 039 S Balkan Frontier A Political Study of The Northern Balkans 900 1204Balázs Dóczi100% (13)
- 2007Dokument6 Seiten2007api-302133133Noch keine Bewertungen
- A Guide for the Psychosocial Treatment of InfertilityVon EverandA Guide for the Psychosocial Treatment of InfertilityNoch keine Bewertungen
- The Zoe Panel As A Reflection of Change in Eleventh-Century ByzantiumDokument17 SeitenThe Zoe Panel As A Reflection of Change in Eleventh-Century ByzantiumVictor Hugo Esquivel100% (1)
- OB Journal Post Partum DepressionDokument11 SeitenOB Journal Post Partum DepressionJames MontemayorNoch keine Bewertungen
- Depresia Postpartum PDFDokument25 SeitenDepresia Postpartum PDFAndreea Tararache100% (1)
- Maternal Mental Health During PregnancyDokument25 SeitenMaternal Mental Health During PregnancyAfrose FathimaNoch keine Bewertungen
- Mental Health Problems During Pregnancy and The Postpartum Period A Multicenter Knowledge Assessment Survey Among Healthcare ProvidersDokument7 SeitenMental Health Problems During Pregnancy and The Postpartum Period A Multicenter Knowledge Assessment Survey Among Healthcare ProvidersRifaniNugrohoNoch keine Bewertungen
- Depression Screening During PregnancyDokument5 SeitenDepression Screening During PregnancyLuvastranger Auger100% (1)
- Postpartum Depression Essay ThesisDokument9 SeitenPostpartum Depression Essay Thesisafcmfuind100% (2)
- NIH Public Access: Management of Postpartum DepressionDokument20 SeitenNIH Public Access: Management of Postpartum DepressionLanny ArmanNoch keine Bewertungen
- Depression During Pregnancy Rates Risks and Consequences Motherisk Update 2008Dokument8 SeitenDepression During Pregnancy Rates Risks and Consequences Motherisk Update 2008Lastry WardaniNoch keine Bewertungen
- General Hospital Psychiatry: Psychiatry and Primary CareDokument5 SeitenGeneral Hospital Psychiatry: Psychiatry and Primary CareAndra NicoleNoch keine Bewertungen
- Postpartum Depression DissertationDokument7 SeitenPostpartum Depression DissertationPaperWritingServiceCheapAnnArbor100% (1)
- Artigo CapacitaçãoDokument14 SeitenArtigo CapacitaçãoKaren AraujoNoch keine Bewertungen
- Wisner Et Al - Antipsychotic Treatment During PregnancyDokument8 SeitenWisner Et Al - Antipsychotic Treatment During PregnancymirasaqqafNoch keine Bewertungen
- Literature Review On Postpartum DepressionDokument5 SeitenLiterature Review On Postpartum Depressionea6bmkmc100% (1)
- Literature Review On Perinatal DepressionDokument6 SeitenLiterature Review On Perinatal Depressionc5rf85jq100% (1)
- Research PaperDokument15 SeitenResearch Paperapi-738831252Noch keine Bewertungen
- Depresión Perinatal en PadresDokument18 SeitenDepresión Perinatal en PadresClaudio Esteban PicónNoch keine Bewertungen
- Lit Review Visual FinalDokument1 SeiteLit Review Visual Finalapi-340988574Noch keine Bewertungen
- Research Paper Postpartum DepressionDokument6 SeitenResearch Paper Postpartum Depressionafedonkfh100% (1)
- Lit Review Postpartum Depression PDFDokument289 SeitenLit Review Postpartum Depression PDFMulti Sri MegawatiNoch keine Bewertungen
- Postnatal Depression Dissertation IdeasDokument5 SeitenPostnatal Depression Dissertation IdeasWhoWillWriteMyPaperForMeCanada100% (1)
- Literature Review Postnatal DepressionDokument5 SeitenLiterature Review Postnatal Depressionafdtftloi100% (1)
- Antenatal Psychosocial Risk Status and Australian Women's Use of Mrimary CareDokument13 SeitenAntenatal Psychosocial Risk Status and Australian Women's Use of Mrimary CareRamzijaNoch keine Bewertungen
- (Asian Biomedicine) Perinatal Depression in Asian Women Prevalence Associated Factors and Cultural AspectsDokument15 Seiten(Asian Biomedicine) Perinatal Depression in Asian Women Prevalence Associated Factors and Cultural AspectsIntan Hajar FauzaninNoch keine Bewertungen
- E Table of Contents. Postpartum Psychosis: The Role of Women's Health Care Providers and The Health Care SystemDokument15 SeitenE Table of Contents. Postpartum Psychosis: The Role of Women's Health Care Providers and The Health Care System4mdw25zqghNoch keine Bewertungen
- Tugas JurnalDokument20 SeitenTugas JurnalHans BasriNoch keine Bewertungen
- Postnatal Depression ThesisDokument6 SeitenPostnatal Depression Thesisangelashfordmurfreesboro100% (2)
- Post Partum DepressiomDokument8 SeitenPost Partum DepressiomSiti Habibah ZeinNoch keine Bewertungen
- Postpartum Depression Research Paper OutlineDokument4 SeitenPostpartum Depression Research Paper Outlinetrvlegvkg100% (1)
- 1471 2458 10 499Dokument15 Seiten1471 2458 10 499Cátia Alexandra CorreiaNoch keine Bewertungen
- Postpartum Depression in Asian Cultures A Literature ReviewDokument8 SeitenPostpartum Depression in Asian Cultures A Literature Reviewgvzfmq91Noch keine Bewertungen
- Postpartum Depression ThesisDokument4 SeitenPostpartum Depression Thesisangelalovettsavannah100% (1)
- Depresion Posaborto 2Dokument7 SeitenDepresion Posaborto 2ESE HOSPITAL SAN PEDRO CLAVERNoch keine Bewertungen
- Mood and Anxiety Disorders in Pregnant and Postpartum Women: PositionDokument7 SeitenMood and Anxiety Disorders in Pregnant and Postpartum Women: PositionMuhammad rizalNoch keine Bewertungen
- Journal 11Dokument5 SeitenJournal 11Francis GecobeNoch keine Bewertungen
- Midwifery Dissertation Postnatal DepressionDokument8 SeitenMidwifery Dissertation Postnatal DepressionCollegePaperHelpCanada100% (1)
- AbortoDokument6 SeitenAbortoS bmNoch keine Bewertungen
- What Can Cause Postpartum Depression - EditedDokument7 SeitenWhat Can Cause Postpartum Depression - EditedkimsmakicheNoch keine Bewertungen
- Depression During PregnancyDokument3 SeitenDepression During PregnancySellymarlinaleeNoch keine Bewertungen
- DepressionDokument5 SeitenDepressionapi-336702702Noch keine Bewertungen
- Sleeping 1Dokument9 SeitenSleeping 1sarah gillNoch keine Bewertungen
- Literature Review of Risk Factors and Interventions On Postpartum DepressionDokument7 SeitenLiterature Review of Risk Factors and Interventions On Postpartum DepressionafmzhpeloejtzjNoch keine Bewertungen
- The Impact of Partner Support in The Treatment of Postpartum Depression (2000)Dokument6 SeitenThe Impact of Partner Support in The Treatment of Postpartum Depression (2000)Iona KalosNoch keine Bewertungen
- Who Paper Depression WFMH 2012Dokument3 SeitenWho Paper Depression WFMH 2012analailaNoch keine Bewertungen
- Nursing Children and Adolescents With Bipolar Disorder: Assessment, Diagnosis, Treatment, and ManagementDokument8 SeitenNursing Children and Adolescents With Bipolar Disorder: Assessment, Diagnosis, Treatment, and ManagementmeronayezabuNoch keine Bewertungen
- Increasing Incidence of Depression in Australia Causes and TreatmentDokument10 SeitenIncreasing Incidence of Depression in Australia Causes and TreatmentAsad BilalNoch keine Bewertungen
- Thesis For Depression Research PaperDokument7 SeitenThesis For Depression Research Papergj9zvt51100% (2)
- Literature Review Postpartum Depression FinalDokument14 SeitenLiterature Review Postpartum Depression Finalapi-730811728Noch keine Bewertungen
- Induced Abortion and Mental Health Systematic Review Consultation - 6 April To 29 June 2011 Comments and ResponsesDokument308 SeitenInduced Abortion and Mental Health Systematic Review Consultation - 6 April To 29 June 2011 Comments and ResponsesMarthasWisdomNoch keine Bewertungen
- Perinatal Mental Illness 2014Dokument10 SeitenPerinatal Mental Illness 2014Julia SenturiónNoch keine Bewertungen
- Perinatal Predictors of Postpartum Depression: Results of A Retrospective Comparative StudyDokument11 SeitenPerinatal Predictors of Postpartum Depression: Results of A Retrospective Comparative StudyDewi NofiantiNoch keine Bewertungen
- Psychopharmacology and Pregnancy: Treatment Efficacy, Risks, and GuidelinesVon EverandPsychopharmacology and Pregnancy: Treatment Efficacy, Risks, and GuidelinesNoch keine Bewertungen
- Tannous Syria Between Byzantium and IslamDokument652 SeitenTannous Syria Between Byzantium and IslamVictor Hugo Esquivel100% (1)
- Identification of The Byzantine Encaustic Mural Painting in EgyptDokument14 SeitenIdentification of The Byzantine Encaustic Mural Painting in EgyptVictor Hugo EsquivelNoch keine Bewertungen
- A-M Talbot ST Mary of EgiptDokument30 SeitenA-M Talbot ST Mary of EgiptDan GeorgescuNoch keine Bewertungen
- Tannous Syria Between Byzantium and IslamDokument652 SeitenTannous Syria Between Byzantium and IslamVictor Hugo Esquivel100% (1)
- Jjarnold 1Dokument304 SeitenJjarnold 1Victor Hugo EsquivelNoch keine Bewertungen
- The Battle of The MastsDokument5 SeitenThe Battle of The MastsVictor Hugo EsquivelNoch keine Bewertungen
- Battle of The Gates of TrajanDokument6 SeitenBattle of The Gates of TrajanVictor Hugo EsquivelNoch keine Bewertungen
- Sex Crimes in ByzantiumDokument3 SeitenSex Crimes in ByzantiumVictor Hugo EsquivelNoch keine Bewertungen
- Home Visit PlanDokument2 SeitenHome Visit Planako at ang exoNoch keine Bewertungen
- Mrs. Shwetha Rani C.MDokument38 SeitenMrs. Shwetha Rani C.MSanthosh.S.UNoch keine Bewertungen
- 1471 2393 14 80 PDFDokument5 Seiten1471 2393 14 80 PDFPaula PebriantyNoch keine Bewertungen
- Postpartum: "Maternal Care - Lecture"Dokument3 SeitenPostpartum: "Maternal Care - Lecture"RAYNELAH ANN NONANNoch keine Bewertungen
- Mercy Obstetric Triage OTDA A Standardised Approach To Care CHA SlidesDokument28 SeitenMercy Obstetric Triage OTDA A Standardised Approach To Care CHA Slidessaepulloh bin amingNoch keine Bewertungen
- 429 FT0 Physiotherapy in Obstetrics Gynaecology Mohd. JavedDokument86 Seiten429 FT0 Physiotherapy in Obstetrics Gynaecology Mohd. JavedRekha Satheesan100% (1)
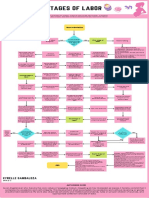
- Stages of Labor FlowchartDokument1 SeiteStages of Labor FlowchartXyrelle GambalozaNoch keine Bewertungen
- MCQ's Knust-1Dokument43 SeitenMCQ's Knust-1Khobby JoeNoch keine Bewertungen
- Returning To Running Postnatal - Guidelines For Medical, Health and Fitness Professionals Managing This PopulationDokument41 SeitenReturning To Running Postnatal - Guidelines For Medical, Health and Fitness Professionals Managing This PopulationHưng LêNoch keine Bewertungen
- Study Guide For Postpartal Care-Module 7Dokument3 SeitenStudy Guide For Postpartal Care-Module 7annyeong_123Noch keine Bewertungen
- Breast Feeding Problems in Primipara Mothers in Early Postnatal Period Bushra Najem Lamia Dhia Al-DeenDokument4 SeitenBreast Feeding Problems in Primipara Mothers in Early Postnatal Period Bushra Najem Lamia Dhia Al-DeenEstellaNoch keine Bewertungen
- Postpartum ComplicationsDokument56 SeitenPostpartum Complicationsjennifer sampangNoch keine Bewertungen
- Obstetric PalsyDokument4 SeitenObstetric PalsyDelphy VargheseNoch keine Bewertungen
- Jurnal Reading - CIndyDokument15 SeitenJurnal Reading - CIndyCindy ElvinaNoch keine Bewertungen
- History ObgynDokument37 SeitenHistory ObgynRana WaelNoch keine Bewertungen
- Acute Pain - Teaching Care PlanDokument4 SeitenAcute Pain - Teaching Care PlanFeliza Therese A. DeloriaNoch keine Bewertungen
- Questionnaire GYN ENG - OMLDokument14 SeitenQuestionnaire GYN ENG - OMLJesus Mosquera LopezNoch keine Bewertungen
- Rle 107 Maternal and Child Health Nursing: University of The Assumption College of Nursing and PharmacyDokument6 SeitenRle 107 Maternal and Child Health Nursing: University of The Assumption College of Nursing and PharmacyEvangeline Anne MacanasNoch keine Bewertungen
- S3 Perinatal DeppressionDokument15 SeitenS3 Perinatal DeppressionAmir Iqbal Mallick100% (1)
- MODULE 5 POSTPARTUM NRG 203 REDOBLE TANUTAN CHAVEZ and FELEODokument24 SeitenMODULE 5 POSTPARTUM NRG 203 REDOBLE TANUTAN CHAVEZ and FELEONyze GarrixNoch keine Bewertungen
- McNaughton-2004-Public Health Nursing PDFDokument13 SeitenMcNaughton-2004-Public Health Nursing PDFasmauryanahNoch keine Bewertungen
- MOH 515 Updated 2022Dokument1 SeiteMOH 515 Updated 2022MARTIN100% (3)
- WHO Working Paper #2Dokument2 SeitenWHO Working Paper #2Vaibhav PenukondaNoch keine Bewertungen
- Case Report Uterine InversionDokument64 SeitenCase Report Uterine InversionFelicia Yumita Winata100% (1)