Beruflich Dokumente
Kultur Dokumente
Epidemiology of Tuberculosis
Hochgeladen von
Amrina RosyadaCopyright
Verfügbare Formate
Dieses Dokument teilen
Dokument teilen oder einbetten
Stufen Sie dieses Dokument als nützlich ein?
Sind diese Inhalte unangemessen?
Dieses Dokument meldenCopyright:
Verfügbare Formate
Epidemiology of Tuberculosis
Hochgeladen von
Amrina RosyadaCopyright:
Verfügbare Formate
Epidemiology of tuberculosis
INTRODUCTION An understanding of the epidemiology of Mycobacterium tuberculosis is critical for effective control. The global burden of tuberculosis (TB), risk factors for transmission, and the epidemiology of TB in the United States will be reviewed here. The epidemiology of drug-resistant TB is discussed separately. COMPLEX M.
(26 to 100 cases/100,000) occur in Central and South America, Eastern Europe, and northern Africa. Low rates (less than 25 cases per 100,000 inhabitants) occur in the United States, Western Europe, Canada, Japan, and Australia. Poverty, HIV, and drug resistance are major contributors to the resurging global TB epidemic [5,6]. Approximately 95 percent of TB cases occur in developing countries. Approximately 1 in 14 new TB cases occur in individuals who are infected with HIV; 85 percent of these cases occur in Africa [3]. An estimated half million cases of multidrug resistant (MDR)-TB also occur annually in Africans; even higher rates of the
M.
TUBERCULOSIS
tuberculosis
is
member
of
drug resistant disease occur in Eastern Europe. Strategies and targets for control After decades of relative neglect, global efforts to control TB were reinvigorated in 1991 when a World Health Assembly resolution recognized TB as a major global health problem [7]. The five-element DOTS (Directly Observed Therapy, Short-course) strategy was developed by the WHO as a response in the mid 1990s; the components included [8,9]: Government commitment to TB control Case detection among symptomatic patients Standardized chemotherapy for all sputum smear-positive cases under proper case management conditions
Mycobacterium tuberculosis complex; other members include Mycobacterium africanum and Mycobacterium bovis. M. africanum is most commonly found in West African countries; it causes up to a quarter of cases of tuberculosis (TB) in the Gambia [1]. The symptoms of infection resemble those of M. tuberculosis. The infectivity is similar to M. tuberculosis, and it is an important opportunistic pathogen in the setting of advanced
immunosuppression due to HIV or other causes. Management is identical to management for disease due to M. tuberculosis. M. bovis is discussed in detail separately. GLOBAL BURDEN More than 2 billion people (about one-third of the world population) are estimated to be infected with Mycobacterium tuberculosis [2]. The global incidence of tuberculosis (TB) peaked around 2003 and appears to be declining slowly [3]. According to the World Health Organization (WHO), in 2010, 8.8 million individuals became ill with TB and 1.4 million died [4]. Both these statistics reflect a decline compared with prior years. The number of individuals infected with TB peaked in 2005, when 9 million individuals became ill. The death peaked at 1.8 million in 2003. The epidemiology of TB varies substantially around the world (figure 1 and table 1). The highest rates (100/100,000 or higher) are observed in sub-Saharan Africa, India, China, and the islands of Southeast Asia and Micronesia. Intermediate rates of TB
Regular drug supply Monitoring system for program supervision and evaluation The DOTS framework was subsequently implemented in 184 countries. This change vastly improved the quality and outreach of national TB programs. By 2006 over 25 of the 32 million patients treated in DOTS programs worldwide were cured [3]. Several challenges emerged during the implementation of DOTS that were not fully addressed in the original World Health Assembly recommendations. To address these problems, a new plan entitled Stop TB Partnership: The Global Plan to Stop TB 2006-2015 was developed by the WHO [10-13]. In addition to enhancing the original elements of DOTS (with a stronger focus on diagnostic accuracy and
patient-centered treatment adherence), the following additional control components included: Collaborative activities implemented jointly by TB and HIV/AIDS programs New treatment strategies to manage MDR-TB New community approaches to engage all relevant partners in national TB program implementation, for expansion of equitable access to diagnosis and treatment Health system strengthening to address impediments to national TB program implementation (eg, limited human resources, financial and managerial capabilities) The Global Drug Facility and the Green Light Committee were formed to improve global access to affordable and quality-assured first- and secondline drugs [14,15]. Intensified research to develop better TB diagnosis, prevention and treatment tools
Other important goals (not explicitly included in the above programs) include reducing the number of patients with infected with strains of MDR-TB, increasing the number of TB patients who are tested for HIV, increasing the number of HIV-infected TB patients enrolled on antiretroviral treatment, and increasing the number of HIVinfected individuals enrolled in treatment for latent TB infection. Progress toward targets Progress has been made in achieving the first MDG target (to halt and reverse rising trends in the incidence of TB). This goal has been wholly or partially achieved in most regions of the world [3]. There has been less success in achieving the second MDG target (to halve the prevalence and death rates due to TB present in 1990 by the year 2015). However, some progress has been achieved. For example, if the rate of improvement seen from 2001-2006 in prevalence and death rates in the Americas, eastern Mediterranean, Southeast Asia and western Pacific regions continues during the period 2006 and 2014, the second MDG goal will be achieved. Unfortunately, this goal will not be achieved by 2015 in the African and European regions at the current
These components were designed to address new "Millennium Development Goals" (MDG) for TB control and prevention. These goals are as follows [13]: To halt and reverse the trend of rising incidence of TB by 2015 To halve the 1990 prevalence of TB and death rates due to TB by 2015 To reduce the worldwide incidence of TB to 1 per million by 2050 Epidemiologists have used mathematical models to predict that detection of at least 70 percent of the incident cases of infectious TB and cure of at least 85 percent of cases are needed to reduce TB incidence, prevalence, and death [16,17]. Therefore, the two most important targets for achieving TB control are to detect at least 70 percent of new TB cases and to achieve a treatment success rate of 85 percent [3]. However, the models mentioned above do not account for common and real problems such as treatment delays, relapses, or changes in vulnerability to infection or strain virulence.
rates of improvement. One difficulty in achieving the goals described is that a dramatic TB resurgence occurred in some areas during the 1990s. In Africa, this resurgence was largely due to the HIV epidemic, but it was also compounded by poor access to health services [18]. In Eastern Europe, this resurgence can be attributed to widespread economic decline, secondary declines in the overall quality of health services, poor living conditions, alcoholism, and the emergence of infection due to MDR strains of M. tuberculosis [19,20]. The third MDG target (to reduce the incidence of TB to <1 case per million by 2050) appears to be unachievable at this time. An annual decline of 15 percent in the worldwide incidence of TB is required to meet this goal. Even with complete implementation of all the control measures advocated by the World Health Agency, the third MDG target goal cannot be achieved by 2050.
As noted above, the two most important targets for TB control have been to reach at least 70 percent case detection and 85 percent treatment success [3]. Case detection rates are highest in western Pacific, Americas, and Southeast Asia (68 to 70 percent) and lowest in Africa, Europe, and the eastern Mediterranean (46 to 52 percent). Asia and Africa account for the majority of global cases of TB (55 and 31 percent, respectively). Two thirds of the "missing cases" occur in China, India, and Africa [3]. Data on treatment success rates follow similar geographic patterns, although these rates reflect only the proportion of patients who received treatment. It is sometimes uncertain whether these patients completed an effective treatment course. The western Pacific, Americas, and Southeast Asia have had the greatest success (78 to 92 percent); Africa, Europe, and the eastern Mediterranean have fared less well (70 to 83 percent). Success is limited in part by the high prevalence of HIV infection in Africa and drug resistance in Eastern Europe. Most patients who are coinfected with TB and HIV are not recognized to be coinfected. For example, the worldwide percentage of patients with TB disease who underwent subsequent HIV testing improved only marginally (from 1 to 12 percent) during the time periods 2002 to 2006. The significance of this failure to test for TB/HIV coinfection is important, as the proportion of coinfected patients has risen steeply in sub-Saharan Africa [21-23]. In Zimbabwe, for example, the number of patients treated for TB increased 10-fold from the 1980s to 2005 [23]. Yet only 22 percent of the patients from Zimbabwe identified as having TB during this time span underwent testing for HIV coinfection, despite the fact that Zimbabwe has been known to have a high prevalence of HIV for decades. The authors of the preceding study estimated that approximately one in four Zimbabwean patients coinfected with HIV and TB was identified as coinfected. Detection and treatment of MDR-TB is also inadequate. Among the patients tested in 27 countries with high rates of MDR-TB, only about 5 percent of the estimated number of MDR-TB cases in these countries were identified [3]. Treatment rates
range from 60 to 69 percent in countries with programs endorsed by the Green Light Committee (GLC) and 28 to 36 percent in countries without GLC-approved projects [3]. As noted above, however, these treatment rates reflect only the proportion of patients who received treatment; it is uncertain whether these patients completed an effective treatment course. Socioeconomic factors Socioeconomic development and access to quality of health services appear to be at least as important as any specific TB control measure. The likelihood of success of TB control efforts is likely related to socioeconomic indicators, including gross domestic product per capita, mortality of children <5, access to clean water, and adequate sanitation and health expenditure per capita. The importance of addressing these socioeconomic factors to achieve TB control is reinforced by the fact that many countries have experienced a rapid decline in TB burden without good access to high-quality TB treatment. In Europe, for example, TB morbidity and mortality declined long before effective chemotherapy was available, largely because of socioeconomic development, improved living conditions, better nutrition, and isolation of infectious cases in sanatoria [24]. RISK FACTORS Risk factors for TB may be divided as follows: Impaired immunity (host factors) Increased exposure to infection (environmental factors) Host factors Categories of host factors are outlined in the following sections. The relative risk for selected risk factors is outlined below. The relative importance of different risk factors varies with prevalence of exposure across regions. Substance abuse Substance abuse is the most commonly reported behavioral risk factor among patients with TB in the United States [50].
Drug use The epidemiologic factors associated with injection and noninjection drug use (eg, homelessness, incarceration) contribute to the high prevalence of TB among drug users [51-56]. Tobacco Cigarette smoking confers a relative risk of about 1.5 to 2.0 for the development of tuberculosis (TB) [57,58]. Smoking has been found to be associated with both risk of relapse of TB and TB mortality. Passive smoking also increases the risk for TB [59]. Alcohol The risk of active TB is substantially elevated in individuals who consume more than 40 g alcohol per day [60]. This may be due to the effect of alcohol and alcohol-related conditions on the immune system. Nutritional status Malnutrition is generally understood to be an important risk factor for TB, although the relation between impaired immunity due to malnutrition and risk of acquiring TB has not been well characterized [61-65]. Underweight Persons who are underweight (body mass index of <18.5) have increased risk for TB by a factor of 2.6 (1.2 to 4.8) [61,62]. Vitamin D Vitamin D plays an important role in macrophage activation and restriction of mycobacterial growth, and diminished serum vitamin D levels appear to increase risk for TB infection [66-71]. Among African immigrants in Australia, for example, individuals with latent or active TB were observed to have substantially lower serum vitamin D levels than those without TB [70]. Iron status Iron is an important growth factor for M. tuberculosis in macrophages and appears to play an important role in host susceptibility to TB infection [72]. Systemic diseases The diseases discussed in this section have been noted to confer some degree of increased risk for TB reactivation. However, in some cases it can be difficult to discern the relative risk of systemic diseases for development of
active TB, since many studies were performed in areas where the prevalence of TB is relatively low. Silicosis The risk of TB is increased among miners with silicosis. The mechanism is not fully understood but may be related to impairment of pulmonary macrophage function by silica crystals. The relative risk depends on the severity of the silicosis and has been estimated at 1.4 to 2.9 [73-75]. Malignancy The risk of TB is increased in patients with hematologic malignancies and head and neck cancer [76]. In a 25 year review of cancer patients in the United States, the rate of TB among patients with hematologic neoplasms was >200 cases per 100,000 persons, or about 40 times the rate among the general population. Among patients with head and neck cancer, the rate was >100 cases per 100,000 persons. It is important to note that these studies were performed in areas where the prevalence of TB is relatively low. Patients with solid tumors other than head and neck cancer do not have an increased risk for TB; among these individuals the rate paralleled that of the general population. Diabetes The risk of developing tuberculosis increases with increasing diabetes severity [77]. A case control study of 5290 patients demonstrated that poorly controlled diabetes confers a 2.9-fold increase in the risk of developing pulmonary TB; the risk associated with well-controlled diabetes was minimal [78]. The mechanism by which diabetes confers an altered immune response to M. tuberculosis is not fully understood but may be related in part to altered cytokine expression [79]. Renal disease The risk of TB among patients with chronic renal disease risk is 6.9 to 52.5 times that of individuals without renal disease [80,81]. Uremia causes reduced cellular immunity. Other factors that may diminish immunity in the setting of renal failure include malnutrition, vitamin D deficiency, and hyperparathyroidism.
Gastric surgery Gastric resection for peptic ulcer disease has been described as a risk factor for TB (relative risk 1.7 to 2.0) [82,83]. Although this procedure is no longer performed routinely, gastric bypass is a similar procedure that may confer similar risk [84]. The mechanism is not understood but may be related to loss of gastric acidity; however, the risk of TB among persons with gastric achlorhydria has not been studied. Celiac disease Celiac disease (autoimmune inflammation of the small intestine) is a risk factor for TB; the mechanism is not fully understood but may be related to malabsorption [85]. In a study of two national registries, the risk of TB was significantly higher among 14,335 individuals with a prior diagnosis of celiac disease than among the 69,888 matched controls (hazard ratio 3.74).
Transplant Renal, cardiac, liver, and allogeneic stem cell transplants are all associated with increased risk for TB [93-96]. The risk in allogeneic stem cell transplants is less than in solid organ transplant patients; there does not appear to be an increased risk of TB in autologous stem cell transplant patients.
Age and gender Age In the developing world TB rates are highest among young adults, reflecting primary transmission in this age group. In the United States and other developed countries, the rate of TB among the elderly is higher than among younger adults and children, reflecting reactivation disease, possibly attributable to impaired immunity with aging. Gender The rate of TB is higher among men than women, beginning in
Immune compromise HIV HIV infection markedly increases the risk for primary and reactivation TB; the magnitude of risk is likely variable depending on the degree of HIVinduced immunosuppression [18,27,78,86]. Among HIV-seropositive
the young adult years and persisting throughout life. This is a longstanding observation thought to reflect more frequent TB exposure in the community among men than women [97].
individuals the risk of acquiring TB is 9 to16 times that of HIV-seronegative individuals [87,88]. The risk of TB decreases with initiation of antiretroviral therapy [89,90]. Glucocorticoids Patients receiving a daily dose of 15 mg
Social and environmental factors Household contacts Close household contact with an individual with smearpositive pulmonary TB is the most important risk factor for TB [11,98]. In a study of TB contact investigation including 1080 smear-positive patients and their 6225 close contacts, 36 percent of contacts had positive tuberculin skin tests [99]; this compares to an expected skin-test positive rate of only 2.9 percent in the general population [49]. Birth in a TB-endemic area The fraction of TB cases in the United States ascribed to foreign born individuals increased from 22 to 58 percent between 1986 and 2007 (figure 4) [36,100]. The risk of TB is highest in the first five years after immigration, but remains higher than the United States-born population for up to 20
of prednisone (or its equivalent) for 1 month are at increased risk for TB [91]. A case-control study in the United Kingdom including more than 16 million person-years of TB risk demonstrated that patients with TB were 4.9 times more likely to have been using glucocorticoids than those without TB [92]. TNF inhibitors Tumor necrosis factor (TNF)-alpha inhibitors (used in the treatment of rheumatic diseases and inflammatory bowel disease) impair host resistance to TB. This issue is discussed in detail separately.
years after arrival [43]. Seven countries account for the majority of cases of TB in foreign-born persons in the United States: Mexico, the Philippines, Vietnam, India, and China, the Dominican Republic and Haiti [43,100,101]. Overseas screening for TB among United States-bound immigrants and refugees is a high-yield intervention for identifying TB and could reduce the number of TB cases among foreign-born persons in the United States [102]. Between 1999 and 2005, the prevalence of smear negative and latent TB cases among immigrants was 961 and 837 cases per 100,000, respectively; the prevalence of these entities among refugees was 1036 and 2838 per 100,000 respectively. Active pulmonary TB and latent TB were diagnosed in the United States in 7 and 1.6 percent of those with overseas diagnoses, respectively. Community settings In places where contact with infectious individuals may occur, risk for acquiring TB infection is increased. Crowding and poor ventilation can increase the risk of transmission in such settings [103-110]. Those at risk for increased exposure include residents and employees of congregate settings such as hospitals, correctional facilities, nursing homes, and homeless shelters. Among 1289 inmates incarcerated in 16 Maryland prisons in 1997, the incidence of tuberculin skin conversion was 6.3 infections per 100 person-years [103]. status TB SUMMARY More than 2 billion people (about one-third of the world population) are estimated to be infected with tuberculosis (TB). The global incidence of TB peaked around 2003 and appears to be been declining slowly. In 2006 the World Health Organization (WHO) estimated that the prevalence of active disease was 14.4 million, a prevalence rate of 219/100,000 persons. The incidence of new cases was 9.2 million, an incidence rate of 139/100,000. Poverty, HIV and drug resistance fan the flames of the TB epidemic. Worldwide, about 95 percent of TB cases occur in developing countries. Among all new TB cases in 2006, about 7 percent were estimated to be HIV infected; 85 percent of these cases occur in Africa. In that year there were an estimated half million cases of multidrug resistant (MDR)-TB; the rate was highest in Eastern Europe. The five-element DOTS (Directly Observed Therapy, Short-course) strategy was developed by WHO in the mid 1990s. To address several challenges emerged during the implementation of DOTS, a new plan entitled Stop TB Partnership: The Global Plan to Stop TB 2006-2015 was outlined by the WHO. Socioeconomic has traditionally been associated with low The first Millennium Development Goals (MDG) target (to halt and reverse TB incidence) has likely been met in most regions, although the other two MDG targets (to halve 1990 prevalence and death rates by 2015 and to reduce TB incidence to 1 per million by 2050) are greater challenges. Socioeconomic development and access and quality of health services Minority groups TB disease rates among racial and ethnic minority groups are 5 to 10 times higher than among whites; these groups comprised 83 percent of all reported TB cases in 2007 [37]. Among non-Hispanic whites, Hispanics, nonHispanic blacks and Asians, rates were 1.1, 8.4, 9.3 and 25.8 per 100,000, respectively. appear to be at least as important as any specific TB control measure. Risk factors for TB may be divided into issues related to host immunity (eg, immunologic defects that lead to increased susceptibility to infection) and issues related to environmental exposure to infection (eg, risk of exposure to a case of infectious TB).
socioeconomic status, which also may be associated with crowding, poor nutrition, poor access to medical care, public assistance, unemployment, and low education [111].
17. 1. REFERENCES de Jong BC, Antonio M, Gagneux S. Mycobacterium africanum--review of an important cause of human tuberculosis in West Africa. PLoS Negl Trop Dis 2010; 4:e744. Lnnroth K, Raviglione M. Global epidemiology of tuberculosis: prospects for control. Semin Respir Crit Care Med 2008; 29:481. WHO. Global Tuberculosis control. WHO/HTM/TB/2008.393. Geneva: World Health Organization; 2008. http://www.who.int/tb/publications/global_report/2008/en/index.html (Accessed on December 08, 2011). The WHO Global tuberculosis control report. http://bit.ly/rlO0ti. (Accessed on January 16, 2012). Corbett EL, Marston B, Churchyard GJ, De Cock KM. Tuberculosis in subSaharan Africa: opportunities, challenges, and change in the era of antiretroviral treatment. Lancet 2006; 367:926. Wright A, Zignol M, Van Deun A, et al. Epidemiology of antituberculosis drug resistance 2002-07: an updated analysis of the Global Project on Anti-Tuberculosis Drug Resistance Surveillance. Lancet 2009; 373:1861. WHO. Forty-fourth World Health Assembly. WHA44/1991/REC/1. Geneva: WHO; 1991. Raviglione MC, Pio A. Evolution of WHO policies for tuberculosis control, 1948-2001. Lancet 2002; 359:775. WHO. WHO Tuberculosis Programme-Framework for Effective Tuberculosis Control http://www.who.int/tb/publications/1994/en/index.html (Accessed on December 08, 2011). Raviglione MC, Uplekar MW. WHO's new Stop TB Strategy. Lancet 2006; 367:952. WHO. The Stop TB Strategy: Building on and Enhancing DOTS to meet the TB-Related Millennium Develpment Goals http://www.who.int/tb/publications/2006/en/ (Accessed on December 08, 2011). Stop TB Partnership. The Global Plan to Stop TB 2006-2015. WHO/HTM/STB/2006.35. Geneva: World Health Organization; 2006a http://www.who.int/tb/publications/2006/en/ (Accessed on December 08, 2011). Maher D, Dye C, Floyd K, et al. Planning to improve global health: the next decade of tuberculosis control. Bull World Health Organ 2007; 85:341. Matiru R, Ryan T. The Global Drug Facility: a unique, holistic and pioneering approach to drug procurement and management. Bull World Health Organ 2007; 85:348. Gupta R, Cegielski JP, Espinal MA, et al. Increasing transparency in partnerships for health--introducing the Green Light Committee. Trop Med Int Health 2002; 7:970. Dye C, Garnett GP, Sleeman K, Williams BG. Prospects for worldwide tuberculosis control under the WHO DOTS strategy. Directly observed short-course therapy. Lancet 1998; 352:1886.
18.
2. 3.
19. 20. 21. 22.
4. 5.
23.
6.
24. 25. 26. 27.
7. 8. 9.
10. 11.
28. 29.
12.
30.
13. 14.
31.
32. 33.
15.
16.
34.
Borgdorff MW, Floyd K, Broekmans JF. Interventions to reduce tuberculosis mortality and transmission in low- and middle-income countries. Bull World Health Organ 2002; 80:217. Corbett EL, Watt CJ, Walker N, et al. The growing burden of tuberculosis: global trends and interactions with the HIV epidemic. Arch Intern Med 2003; 163:1009. Walberg P, McKee M, Shkolnikov V, et al. Economic change, crime, and mortality crisis in Russia: regional analysis. BMJ 1998; 317:312. Leon DA, Chenet L, Shkolnikov VM, et al. Huge variation in Russian mortality rates 1984-94: artefact, alcohol, or what? Lancet 1997; 350:383. Dye C. Global epidemiology of tuberculosis. Lancet 2006; 367:938. Lawn SD, Bekker LG, Middelkoop K, et al. Impact of HIV infection on the epidemiology of tuberculosis in a peri-urban community in South Africa: the need for age-specific interventions. Clin Infect Dis 2006; 42:1040. Corbett EL, Muzangwa J, Chaka K, et al. Nursing and community rates of Mycobacterium tuberculosis infection among students in Harare, Zimbabwe. Clin Infect Dis 2007; 44:317. Lienhardt C. From exposure to disease: the role of environmental factors in susceptibility to and development of tuberculosis. Epidemiol Rev 2001; 23:288. Burzynski J, Schluger NW. The epidemiology of tuberculosis in the United States. Semin Respir Crit Care Med 2008; 29:492. Khan K, Wang J, Hu W, et al. Tuberculosis infection in the United States: national trends over three decades. Am J Respir Crit Care Med 2008; 177:455. Horsburgh CR, Moore M, Castro KG. Epidemiology of tuberculosis in the United States. In: Tuberculosis, 2nd, Rom WN, Garay SM. (Eds), Lippincott Williams and Wilkins, Philadelphia 2004. p.31. Barnes PF, Yang Z, Pogoda JM, et al. Foci of tuberculosis transmission in central Los Angeles. Am J Respir Crit Care Med 1999; 159:1081. Bishai WR, Graham NM, Harrington S, et al. Molecular and geographic patterns of tuberculosis transmission after 15 years of directly observed therapy. JAMA 1998; 280:1679. Alland D, Kalkut GE, Moss AR, et al. Transmission of tuberculosis in New York City. An analysis by DNA fingerprinting and conventional epidemiologic methods. N Engl J Med 1994; 330:1710. Small PM, Hopewell PC, Singh SP, et al. The epidemiology of tuberculosis in San Francisco. A population-based study using conventional and molecular methods. N Engl J Med 1994; 330:1703. Jasmer RM, Hahn JA, Small PM, et al. A molecular epidemiologic analysis of tuberculosis trends in San Francisco, 1991-1997. Ann Intern Med 1999; 130:971. Daley CL, Small PM, Schecter GF, et al. An outbreak of tuberculosis with accelerated progression among persons infected with the human immunodeficiency virus. An analysis using restriction-fragment-length polymorphisms. N Engl J Med 1992; 326:231. Geng E, Kreiswirth B, Driver C, et al. Changes in the transmission of tuberculosis in New York City from 1990 to 1999. N Engl J Med 2002; 346:1453.
35.
36. 37.
38. 39.
40. 41. 42.
43.
44.
45.
46.
47.
48.
49.
50. 51.
Sharnprapai S, Miller AC, Suruki R, et al. Genotyping analyses of tuberculosis cases in U.S.- and foreign-born Massachusetts residents. Emerg Infect Dis 2002; 8:1239. Centers for Disease Control and Prevention (CDC). Trends in tuberculosis-United States, 2008. MMWR Morb Mortal Wkly Rep 2009; 58:249. Centers for Disease Control and Prevention (CDC). Reported HIV status of tuberculosis patients--United States, 1993-2005. MMWR Morb Mortal Wkly Rep 2007; 56:1103. Frieden TR, Fujiwara PI, Washko RM, Hamburg MA. Tuberculosis in New York City--turning the tide. N Engl J Med 1995; 333:229. Centers for Disease Control and Prevention (CDC). Decrease in reported tuberculosis cases - United States, 2009. MMWR Morb Mortal Wkly Rep 2010; 59:289. Centers for Disease Control and Prevention (CDC). Trends in tuberculosis-United States, 2010. MMWR Morb Mortal Wkly Rep 2011; 60:333. Centers for Disease Control and Prevention (CDC). Trends in tuberculosis United States, 2011. MMWR Morb Mortal Wkly Rep 2012; 61:181. Centers for Disease Control and Prevention (CDC). Assessment of declines in reported tuberculosis cases--Georgia and Pennsylvania, 2009. MMWR Morb Mortal Wkly Rep 2011; 60:338. Cain KP, Haley CA, Armstrong LR, et al. Tuberculosis among foreign-born persons in the United States: achieving tuberculosis elimination. Am J Respir Crit Care Med 2007; 175:75. Chin DP, DeRiemer K, Small PM, et al. Differences in contributing factors to tuberculosis incidence in U.S. -born and foreign-born persons. Am J Respir Crit Care Med 1998; 158:1797. Tornieporth NG, Ptachewich Y, Poltoratskaia N, et al. Tuberculosis among foreign-born persons in New York City, 1992-1994: implications for tuberculosis control. Int J Tuberc Lung Dis 1997; 1:528. Borgdorff MW, Behr MA, Nagelkerke NJ, et al. Transmission of tuberculosis in San Francisco and its association with immigration and ethnicity. Int J Tuberc Lung Dis 2000; 4:287. Jasmer RM, Ponce de Leon A, Hopewell PC, et al. Tuberculosis in Mexicanborn persons in San Francisco: reactivation, acquired infection and transmission. Int J Tuberc Lung Dis 1997; 1:536. Walter ND, Jasmer RM, Grinsdale J, et al. Reaching the limits of tuberculosis prevention among foreign-born individuals: a tuberculosis-control program perspective. Clin Infect Dis 2008; 46:103. Bennett DE, Courval JM, Onorato I, et al. Prevalence of tuberculosis infection in the United States population: the national health and nutrition examination survey, 1999-2000. Am J Respir Crit Care Med 2008; 177:348. Oeltmann JE, Kammerer JS, Pevzner ES, Moonan PK. Tuberculosis and substance abuse in the United States, 1997-2006. Arch Intern Med 2009; 169:189. Deiss RG, Rodwell TC, Garfein RS. Tuberculosis and illicit drug use: review and update. Clin Infect Dis 2009; 48:72.
52.
53.
54.
55.
56. 57.
58.
59. 60. 61.
62. 63. 64. 65.
66.
67.
68.
Selwyn PA, Hartel D, Lewis VA, et al. A prospective study of the risk of tuberculosis among intravenous drug users with human immunodeficiency virus infection. N Engl J Med 1989; 320:545. Durante AJ, Selwyn PA, O'Connor PG. Risk factors for and knowledge of Mycobacterium tuberculosis infection among drug users in substance abuse treatment. Addiction 1998; 93:1393. Daley CL, Hahn JA, Moss AR, et al. Incidence of tuberculosis in injection drug users in San Francisco: impact of anergy. Am J Respir Crit Care Med 1998; 157:19. Pevzner ES, Robison S, Donovan J, et al. Tuberculosis transmission and use of methamphetamines in Snohomish County, WA, 1991-2006. Am J Public Health 2010; 100:2481. Gardy JL, Johnston JC, Ho Sui SJ, et al. Whole-genome sequencing and social-network analysis of a tuberculosis outbreak. N Engl J Med 2011; 364:730. Bates MN, Khalakdina A, Pai M, et al. Risk of tuberculosis from exposure to tobacco smoke: a systematic review and meta-analysis. Arch Intern Med 2007; 167:335. Lin HH, Ezzati M, Chang HY, Murray M. Association between tobacco smoking and active tuberculosis in Taiwan: prospective cohort study. Am J Respir Crit Care Med 2009; 180:475. Leung CC, Lam TH, Ho KS, et al. Passive smoking and tuberculosis. Arch Intern Med 2010; 170:287. Lnnroth K, Williams BG, Stadlin S, et al. Alcohol use as a risk factor for tuberculosis - a systematic review. BMC Public Health 2008; 8:289. PALMER CE, JABLON S, EDWARDS PQ. Tuberculosis morbidity of young men in relation to tuberculin sensitivity and body build. Am Rev Tuberc 1957; 76:517. Edwards LB, Livesay VT, Acquaviva FA, Palmer CE. Height, weight, tuberculous infection, and tuberculous disease. Arch Environ Health 1971; 22:106. Tverdal A. Body mass index and incidence of tuberculosis. Eur J Respir Dis 1986; 69:355. Leung CC, Lam TH, Chan WM, et al. Lower risk of tuberculosis in obesity. Arch Intern Med 2007; 167:1297. Cegielski JP, McMurray DN. The relationship between malnutrition and tuberculosis: evidence from studies in humans and experimental animals. Int J Tuberc Lung Dis 2004; 8:286. Chandra G, Selvaraj P, Jawahar MS, et al. Effect of vitamin D3 on phagocytic potential of macrophages with live Mycobacterium tuberculosis and lymphoproliferative response in pulmonary tuberculosis. J Clin Immunol 2004; 24:249. Sita-Lumsden A, Lapthorn G, Swaminathan R, Milburn HJ. Reactivation of tuberculosis and vitamin D deficiency: the contribution of diet and exposure to sunlight. Thorax 2007; 62:1003. Wilkinson RJ, Llewelyn M, Toossi Z, et al. Influence of vitamin D deficiency and vitamin D receptor polymorphisms on tuberculosis among Gujarati Asians in west London: a case-control study. Lancet 2000; 355:618.
69.
70.
71.
72. 73. 74.
75. 76. 77.
78.
79.
80. 81. 82. 83. 84. 85. 86. 87.
Ustianowski A, Shaffer R, Collin S, et al. Prevalence and associations of vitamin D deficiency in foreign-born persons with tuberculosis in London. J Infect 2005; 50:432. Gibney KB, MacGregor L, Leder K, et al. Vitamin D deficiency is associated with tuberculosis and latent tuberculosis infection in immigrants from sub-Saharan Africa. Clin Infect Dis 2008; 46:443. Martineau AR, Nhamoyebonde S, Oni T, et al. Reciprocal seasonal variation in vitamin D status and tuberculosis notifications in Cape Town, South Africa. Proc Natl Acad Sci U S A 2011; 108:19013. Boelaert JR, Vandecasteele SJ, Appelberg R, Gordeuk VR. The effect of the host's iron status on tuberculosis. J Infect Dis 2007; 195:1745. Cowie RL. The epidemiology of tuberculosis in gold miners with silicosis. Am J Respir Crit Care Med 1994; 150:1460. Corbett EL, Churchyard GJ, Clayton TC, et al. HIV infection and silicosis: the impact of two potent risk factors on the incidence of mycobacterial disease in South African miners. AIDS 2000; 14:2759. Kleinschmidt I, Churchyard G. Variation in incidences of tuberculosis in subgroups of South African gold miners. Occup Environ Med 1997; 54:636. Kamboj M, Sepkowitz KA. The risk of tuberculosis in patients with cancer. Clin Infect Dis 2006; 42:1592. Baker MA, Lin HH, Chang HY, Murray MB. The risk of tuberculosis disease among persons with diabetes mellitus: a prospective cohort study. Clin Infect Dis 2012; 54:818. Pablos-Mndez A, Blustein J, Knirsch CA. The role of diabetes mellitus in the higher prevalence of tuberculosis among Hispanics. Am J Public Health 1997; 87:574. Restrepo BI, Fisher-Hoch SP, Pino PA, et al. Tuberculosis in poorly controlled type 2 diabetes: altered cytokine expression in peripheral white blood cells. Clin Infect Dis 2008; 47:634. Hussein MM, Mooij JM, Roujouleh H. Tuberculosis and chronic renal disease. Semin Dial 2003; 16:38. Pien FD, Younoszai BG, Pien BC. Mycobacterial infections in patients with chronic renal disease. Infect Dis Clin North Am 2001; 15:851. THORN PA, BROOKES VS, WATERHOUSE JA. Peptic ulcer, partial gastrectomy, and pulmonary tuberculosis. Br Med J 1956; 1:603. Steiger Z, Nickel WO, Shannon GJ, et al. Pulmonary tuberculosis after gastric resection. Am J Surg 1976; 131:668. Bruce RM, Wise L. Tuberculosis after jejunoileal bypass for obesity. Ann Intern Med 1977; 87:574. Ludvigsson JF, Wahlstrom J, Grunewald J, et al. Coeliac disease and risk of tuberculosis: a population based cohort study. Thorax 2007; 62:23. Havlir DV, Getahun H, Sanne I, Nunn P. Opportunities and challenges for HIV care in overlapping HIV and TB epidemics. JAMA 2008; 300:423. Guelar A, Gatell JM, Verdejo J, et al. A prospective study of the risk of tuberculosis among HIV-infected patients. AIDS 1993; 7:1345.
88.
Antonucci G, Girardi E, Raviglione MC, Ippolito G. Risk factors for tuberculosis in HIV-infected persons. A prospective cohort study. The Gruppo Italiano di Studio Tubercolosi e AIDS (GISTA). JAMA 1995; 274:143. 89. Badri M, Wilson D, Wood R. Effect of highly active antiretroviral therapy on incidence of tuberculosis in South Africa: a cohort study. Lancet 2002; 359:2059. 90. Golub JE, Saraceni V, Cavalcante SC, et al. The impact of antiretroviral therapy and isoniazid preventive therapy on tuberculosis incidence in HIV-infected patients in Rio de Janeiro, Brazil. AIDS 2007; 21:1441. 91. Targeted tuberculin testing and treatment of latent tuberculosis infection. This official statement of the American Thoracic Society was adopted by the ATS Board of Directors, July 1999. This is a Joint Statement of the American Thoracic Society (ATS) and the Centers for Disease Control and Prevention (CDC). This statement was endorsed by the Council of the Infectious Diseases Society of America. (IDSA), September 1999, and the sections of this statement. Am J Respir Crit Care Med 2000; 161:S221. 92. Jick SS, Lieberman ES, Rahman MU, Choi HK. Glucocorticoid use, other associated factors, and the risk of tuberculosis. Arthritis Rheum 2006; 55:19. 93. Lichtenstein IH, MacGregor RR. Mycobacterial infections in renal transplant recipients: report of five cases and review of the literature. Rev Infect Dis 1983; 5:216. 94. Muoz P, Palomo J, Muoz R, et al. Tuberculosis in heart transplant recipients. Clin Infect Dis 1995; 21:398. 95. Meyers BR, Halpern M, Sheiner P, et al. Tuberculosis in liver transplant patients. Transplantation 1994; 58:301. 96. Akan H, Arslan O, Akan OA. Tuberculosis in stem cell transplant patients. J Hosp Infect 2006; 62:421. 97. Comstock GW. Epidemiology of tuberculosis. Am Rev Respir Dis 1982; 125:8. 98. Becerra MC, Appleton SC, Franke MF, et al. Tuberculosis burden in households of patients with multidrug-resistant and extensively drug-resistant tuberculosis: a retrospective cohort study. Lancet 2011; 377:147. 99. Marks SM, Taylor Z, Qualls NL, et al. Outcomes of contact investigations of infectious tuberculosis patients. Am J Respir Crit Care Med 2000; 162:2033. 100. Zuber PL, McKenna MT, Binkin NJ, et al. Long-term risk of tuberculosis among foreign-born persons in the United States. JAMA 1997; 278:304. 101. McKenna MT, McCray E, Jones JL, et al. The fall after the rise: Tuberculosis in the United States, 1991 through 1994. Am J Public Health 1998; 88:1059. 102. Liu Y, Weinberg MS, Ortega LS, et al. Overseas screening for tuberculosis in U.S.-bound immigrants and refugees. N Engl J Med 2009; 360:2406. 103. MacIntyre CR, Kendig N, Kummer L, et al. Impact of tuberculosis control measures and crowding on the incidence of tuberculous infection in Maryland prisons. Clin Infect Dis 1997; 24:1060. 104. Stead WW, Lofgren JP, Warren E, Thomas C. Tuberculosis as an endemic and nosocomial infection among the elderly in nursing homes. N Engl J Med 1985; 312:1483.
105. Schieffelbein CW Jr, Snider DE Jr. Tuberculosis control among homeless populations. Arch Intern Med 1988; 148:1843. 106. Pablos-Mendez A, Raviglione MC, Battan R, Ramos-Zuniga R. Drug resistant tuberculosis among the homeless in New York City. N Y State J Med 1990; 90:351. 107. Centers for Disease Control (CDC). Drug-resistant tuberculosis among the homeless--Boston. MMWR Morb Mortal Wkly Rep 1985; 34:429. 108. Nolan CM, Elarth AM, Barr H, et al. An outbreak of tuberculosis in a shelter for homeless men. A description of its evolution and control. Am Rev Respir Dis 1991; 143:257. 109. Nardell E, McInnis B, Thomas B, Weidhaas S. Exogenous reinfection with tuberculosis in a shelter for the homeless. N Engl J Med 1986; 315:1570. 110. Centers for Disease Control and Prevention (CDC). Tuberculosis outbreak associated with a homeless shelter - kane county, illinois, 2007-2011. MMWR Morb Mortal Wkly Rep 2012; 61:186. 111. Cantwell MF, McKenna MT, McCray E, Onorato IM. Tuberculosis and race/ethnicity in the United States: impact of socioeconomic status. Am J Respir Crit Care Med 1998; 157:1016. Topic 8018 Version 16.0
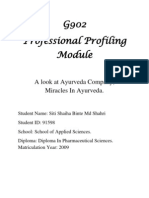
GRAPHICS Estimated TB incidence rates, by country, 2009
Estimated epidemiological burden of TB, 2009* Mortality Population Best 11 83 4.5 10 150 50 54 280 62 6.2 8.8 29 110 60 32 25 23 12 9.3 Low 7.1 60 2.2 7.4 100 36 38 170 36 3.0 6.3 18 89 36 21 17 10 7.2 3.9 High 15 110 8.4 14 220 67 75 430 95 12 12 43 140 93 45 38 44 18 17 Prevalence Best 94 690 100 100 1800 430 480 3000 660 110 86 300 830 640 480 190 390 130 91 Low 43 320 36 47 740 200 220 1300 270 45 43 130 380 270 450 65 160 57 39 High 160 1100 180 170 3000 690 790 5000 1100 190 130 490 1400 1100 510 320 650 210 170 Incidence Best 53 360 87 65 1300 250 300 2000 430 120 94 200 460 420 260 150 490 93 96 Low 43 300 72 56 1100 200 240 1600 350 99 76 160 370 340 210 120 400 75 78 High 64 440 100 76 1500 300 360 2400 520 150 110 240 550 500 310 180 590 110 120 HIV prevalence in incident TB cases (percent) Best -- 0.2 12 6.4 1.5 8.4 12 6.4 2.8 44 58 11 19 1.5 0.5 8 60 17 56 Low -0.1 11 4.5 0.9 6.4 8.8 3.9 1.7 42 58 7.7 19 1.0 0.3 7 54 12 39 High -0.3 12 8.3 2.2 11 15 9.8 4.3 46 58 14 19 2.2 0.8 9 65 22 73
Afghanistan Bangladesh Brazil Cambodia China DR Congo Ethiopia India Indonesia Kenya Mozambique Myanmar Nigeria Pakistan Philippines Russian Federation South Africa Thailand Uganda
28,150 162,221 193,734 14,805 1,345,751 66,020 82,825 1,198,003 229,965 39,802 22,894 50,020 154,729 180,808 91,983 140,874 50,110 67,764 32,710
UR Tanzania Viet Nam Zimbabwe High-burden countries
43,739 88,069 12,523 4,297,498
4.0 32 10 1100
1.5 18 7.5 930
9. 2 50 14 1200
72 290 96 11,000
27 130 48 8900
130 510 150 14,000
80 180 93 7600
75 130 76 7100
85 230 110 8100
47 4.2 52 12
33 2.9 51 11
61 5.8 52 13
Numbers in thousands except where indicated. * Numbers for mortality, prevalence, and incidence shown to two significant figures. Totals for HBCs and globally computed prior to rounding using Monte Carlo simulations. Mortality excludes deaths among HIV-positive TB cases. Deaths among HIV-positive TB cases are classified as HIV deaths according to ICD-10. Best, low, and high indicate best estimates followed by lower and upper bounds. The lower and upper bounds are defined as t he 2.5th and 97.5th centiles of outcome distributions produced in simulations. Indicates no data reported. Bangladesh completed a survey of the prevalence of TB disease in 2009. A reassessment of the epidemiological burden of TB, using data from the survey combined with an in-depth analysis of surveillance and programmatic data, is being undertaken in 2011. Myanmar completed a survey of the prevalence of TB disease in 2010. A reassessment of the epidemiological burden of TB will be undertaken following finalization and dissemination of survey results. Reproduced with permission from: World Health Organization. WHO Report 2010: Global Tuberculosis Control. WHO/HTM/TB/2010.7. Geneva, 2010. Copyright 2010 WHO.
Tuberculosis transmission and control
INTRODUCTION The transmission of tuberculosis (TB) in health care facilities is an important concern. Several outbreaks of nosocomial TB in the United States accompanied the resurgence of the disease in the general population in the late 1980s and early 1990s. Multiple factors contributed to this problem, including deterioration of the public health infrastructure, the human immunodeficiency virus (HIV) epidemic, and inadequate infection control measures in health care facilities. Enhanced infection control measures, as promoted by the Centers for Disease Control and Prevention (CDC) guidelines, have reduced healthcare-associated transmission of TB, and improved public health TB control programs have reduced the incidence of TB in the community as a whole [1]. The 2004 rate was the lowest recorded in the United States since national reporting began in 1953 [1].
HCW training and education regarding TB symptoms, transmission, and prevention Using appropriate signage advising respiratory hygiene and cough etiquette Ensuring proper cleaning and sterilization or disinfection of potentially contaminated equipment (usually endoscopes) Coordinating efforts with the local or state health department GROUPS AT RISK Public health measures and effective chemotherapy have substantially reduced the incidence and prevalence of TB in the United States. Nevertheless, certain segments of the population remain at increased risk of TB, by virtue of having a higher prevalence of infection, a higher risk of progression to active disease if infected, or both. (See "Epidemiology of tuberculosis".) Groups with a higher prevalence of TB infection include [1]: Foreign-born persons from areas with high TB prevalence (especially those
The CDC has identified several key administrative control measures for a successful TB control program [1]: Assigning responsibility for TB infection control Conducting TB risk assessment Developing a written TB infection control plan Early identification and management of patients with TB, including appropriate institution of airborne precautions Environmental control measures, such as the construction and maintenance of airborne infection isolation rooms (AII; previously called negative pressure isolation rooms [NPIR]) Personal protection, including the use of appropriate respirators Ensuring the timely availability of pertinent laboratory testing and reporting of results An effective TB screening program for healthcare workers (HCWs)
who have arrived in the US from endemic areas less than 5 years earlier) and individuals who travel frequently to such areas Homeless or marginally housed persons Residents and employees of congregate settings that are high-risk (eg, correctional facilities, long-term care facilities, and homeless shelters) The elderly (based upon having been alive during a time of higher TB prevalence in the United States) HCWs who serve patients at high risk in the United States HCWs, other professionals, and volunteers who travel abroad to work in healthcare facilities or with refugees in regions in which TB is endemic HCWs with unprotected exposure to a patient with TB disease before the identification and correct airborne precautions of the patient Certain populations who are medically underserved and who have low incomes
Infants, children, and adolescents exposed to adults in high-risk categories Groups with a higher risk of progression to active TB include [1]: Those who have been infected with TB within the previous two years Infants and children younger than four years of age Persons with a history of untreated or inadequately treated TB disease, including those with fibrotic lesions on chest radiography suggestive of healed TB Persons with immunocompromising conditions, including:
TRANSMISSION Person-to-person transmission of TB occurs via inhalation of droplet nuclei (airborne particles 1 to 5 microns in diameter). Coughing and singing facilitate formation of droplet nuclei [2-6]. Persons with active untreated respiratory tract disease (pulmonary or laryngeal) are contagious, particularly when cavitary disease is present or when the sputum is AFB smear positive. However, patients with sputum smear-negative, culture-positive pulmonary TB can transmit infection; among 844 secondary cases of TB in the Netherlands between 1996 and 2004, 13 percent were attributable to transmission from index patients who were smearnegative [7]. Extrapulmonary tuberculosis is not contagious. However, many persons with
HIV infection Hematologic malignancy Cancer of the head, neck and/or lung Organ transplantation Prolonged corticosteroid therapy Treatment with other immunosuppressive agents, such as calcineurin inhibitors, cytotoxic chemotherapeutic agents, and tumor necrosis factor alpha (TNF-alpha) inhibitors Persons with other underlying medical conditions including: Silicosis Diabetes mellitus Chronic kidney disease Gastrectomy or intestinal bypass Body weight 10 percent or more below ideal body weight
extrapulmonary disease also have pulmonary disease; such individuals are contagious. NOSOCOMIAL TRANSMISSION In the late 1980s and early 1990s, multiple urban hospitals in the United States reported outbreaks of TB, involving both patients and HCWs [8-12]. Several of these outbreaks involved multi-drug resistant (MDR)-TB and HIV-infected patients, who have a high risk of developing progressive primary TB. The propensity to develop active TB shortly after initial infection can amplify outbreaks in hospitals or other facilities. At a 32-bed residential facility for HIV-infected persons in San Francisco, for example, 12 cases of active pulmonary TB were diagnosed over a four month period in late 1990 and early 1991; the isolates from the 11 patients with culture-positive disease had similar patterns of restriction fragment length polymorphisms (RFLP) [13,14]. The New York City Department of Health, in response to growing concerns about MDR-TB, investigated all identified cases of TB in the city over a 43 month period starting in January, 1990 [15]. Three hundred and fifty-seven cases of TB resistant to isoniazid, rifampin, ethambutol, and streptomycin were identified; among the 267 cases for which RFLP analysis was available, the patterns were identical or highly
similar. Eighty-six percent of these patients were HIV-infected, and 67 percent were judged likely to have nosocomial TB, acquired at 11 hospitals. Procedures that can result in the dispersal of droplet nuclei have been associated with an increased risk of TB transmission. These include endotracheal intubation, bronchoscopy, sputum induction, aerosol treatments (eg, pentamidine), irrigation of a tuberculous abscess, and autopsy [1]. HEALTHCARE FACILITY POLICIES Hospital TB control programs are critical for limiting nosocomial transmission. A study of skin test (Mantoux test) conversions in HCWs in an urban hospital after the implementation of a TB control program in accordance with CDC guidelines revealed an incidence of 0.38 per 100 personyears worked; 69 of 5773 susceptible employees had a skin test conversion [16]. Immediately prior to the institution of this program, this hospital had measured an annual conversion rate of 13.2 percent among nurses. Development of a TB infection control plan Every healthcare facility should have a written TB infection control plan for each area of the facility and for each occupational group not assigned to a specific area [1]. Periodic risk assessment is essential and should include the following elements: Review of the incidence of TB and affected groups in the community, in collaboration with the local or state department of public health Case surveillance, including tabulation of cases over at least the previous five years Review of drug susceptibility data for TB cases in the facility Determination of which HCWs to include in a TB screening program and respiratory protection program, and at what frequency (see 'Contact investigation' below)
Prompt recognition and evaluation of suspected episodes of healthcareassociated transmission of TB Periodic (preferably annual) assessment of: Proper implementation of the TB infection control plan Prompt identification of suspected cases and initiation of airborne precautions Expert medical management of patients with suspected or confirmed TB disease Pertinent maintenance of environmental controls Recognition and correction of lapses in infection control Early identification of patients with active TB Physicians must be astute in identifying patients who may have active TB, both to benefit the patient and to minimize exposure to HCWs and to other patients. Evaluation should start with a thorough history and physical examination, with attention to epidemiologic risk factors, travel history, and complaints suspicious for active TB, such as persistent (>3 weeks) cough and constitutional symptoms (fever, drenching night sweats, unintentional weight loss). Any hospitalized patient for whom active pulmonary or laryngeal TB is suspected should be placed immediately in an AII room [1]. Relevant risk factors include history of pulmonary TB, previous positive tuberculin skin test result, foreign born status with recent immigration, homelessness, recent incarceration, weight loss and pertinent chest radiograph findings (eg, apical infiltrate or cavitary lesion) [17]. Patients diagnosed with extrapulmonary TB require careful evaluation for pulmonary or laryngeal TB. Immunocompromised patients with extrapulmonary TB should be presumed to have pulmonary TB until proven otherwise with negative sputum samples, even if chest radiography is normal.
The clinical and radiographic presentations of TB are often atypical in persons with impaired cell mediated immunity such as HIV infection and organ transplant recipients [18]. Such patients have an increased frequency of extrapulmonary TB and can have pulmonary disease despite a normal chest x-ray. The diagnosis of pulmonary TB should be pursued with sputum samples for acid-fast smear and mycobacterial culture. If the patient is unable to produce an adequate sample, sputum induction or bronchoscopy should be performed using appropriate precautions. Sample concentration should be employed whenever possible to improve test sensitivity [19] and rapid methods such as fluorescent microscopy should be used to optimize turn-around time; results of acid-fast smears should be available within 24 hours [1]. Nucleic acid amplification testing of positive sputum smears should be employed when possible. Suspected or confirmed cases of TB should be reported promptly to the local public health department in order to expedite contact investigation and to help plan outpatient follow-up. Surveillance for patient-to-patient transmission of TB Routine surveillance of active TB cases should be monitored for clues of patient-to-patient transmission. Clues include a high proportion of cases with prior hospitalizations in the previous year, a sudden increase in cases (especially MDR-TB), or multiple TB patients with identical drug susceptibility patterns (or DNA fingerprint patterns, if available). If suspicion is aroused, HCW tuberculin skin test (TST) or interferon-gamma release assay (IGRA) results and patient surveillance data in the suspected areas should be reviewed for additional cases of active TB or TST/IGRA conversions. Possible contacts between recently diagnosed cases and other patients with active TB should be investigated. If the investigation supports patient-to-patient
transmission, causes for the infection control breakdown should be sought, the possibility of further exposures (patients and HCWs) should be pursued, and the local public health department should be notified [1]. Compliance Multiple studies have been performed to assess compliance with infection control programs for TB in healthcare facilities. One prospective study, which included direct observation in two institutions with MDR-TB found that 19 percent of patients with pulmonary TB were not isolated on their first hospital day, while only 8.6 percent of patients placed into TB isolation proved to have TB [20]. Three to 4.5 percent of individuals did not wear masks to enter the isolation rooms in both institutions, and 50 percent wore surgical masks in one of the hospitals even after N95 respirators became available. In another report, direct observation in three California hospitals determined that 19 percent of patients were placed in rooms that were not designed for negative pressure or in rooms that were not under negative pressure despite being capable of having negative pressure (11 percent) [21]. These studies highlight the need for regular review of compliance with established infection control policies for the control of TB. MANAGEMENT OF SUSPECTED OR CONFIRMED ACTIVE TB Inpatient management Suspicion of active pulmonary TB should prompt placement in an AII room. Such patients should be educated about the purpose of such isolation and instructed to cover their nose and mouth when coughing or sneezing, even when in the room. Whenever possible, procedures should be performed in the AII room to minimize exposure to the rest of the hospital. If the patient must leave the room, a surgical mask must be worn. All other persons entering the room must use respiratory protection, usually an N95 mask [1].
Anti-TB treatment administered during hospitalization should be directly observed therapy (DOT). Transitioning to outpatient management requires careful planning (see below). TB isolation rooms Negative pressure is employed to prevent the escape of droplet nuclei. To accomplish this goal, doors must be kept closed and negative pressure should be verified daily. Anterooms are desirable, but not required; when present, one should not open both the door to the anteroom and the door to the AII room simultaneously. There must be at least six air exchanges per hour; 12 or more exchanges per hour are preferred and are required for any renovation or new construction. Air should be exhausted to the exterior, far removed from any intake vents; if recirculation to general ventilation is unavoidable, HEPA filters must be installed in the exhaust ducts [1]. Respiratory protection masks These masks must filter particles 1 micron in diameter with at least 95 percent efficiency (N95) given flow rates up to 50 L per minute, must fit to a person's face with less than 10 percent seal leakage, and should be available in several sizes to optimize fit. HCW should be fit-tested in order to determine the most appropriate mask size with periodic repeat fit testing [1]. HCWs who are unable to use an N95 mask due to poor fit (eg, bearded individuals and those in whom facial structure precludes a tight seal) should use a powered air purifying respirator (PAPR). Multiple sizes of N95 masks should be available close to AII rooms to ensure proper usage. Controversy exists regarding the appropriate fit testing interval. The Occupational Safety and Health Administration (OSHA) applies the general respiratory protection standard which requires annual fit testing and medical evaluations. However, this standard was designed to protect workers against industrial aerosols, and several medical societies have argued that annual fit testing is not supported by available evidence and is unduly burdensome to healthcare facilities.
Masks should be worn under the following circumstances: Persons entering a TB isolation room when the patient is present Persons present during a cough-inducing or aerosol-inducing procedure on such patients, such as bronchoscopy, induced sputum collection, or administration of aerosolized pentamidine Persons in other settings where administrative and environmental controls are unlikely to be protective (eg, in emergency transport vehicles) [1] These devices are designed to filter air before it is inhaled; thus, patients with known or suspected TB should not wear these masks. Instead, when required to be outside TB isolation rooms, such patients should wear surgical masks, which are designed to prevent the respiratory secretions of the person wearing the mask from entering the environment [1]. Discontinuation of TB isolation A patient may be transferred from an AII room to another hospital room once the diagnosis of TB has been ruled out, or when the patient is being treated for TB and all of the following conditions are met: The patient is on effective therapy The patient is improving clinically Three consecutive sputum samples, obtained on different days, are smearnegative for AFB For patients with initially positive AFB smears, at least two weeks of TB treatment should be administered before isolation is discontinued, although this guideline is somewhat arbitrary and not well supported by data [2,22]. For patients with MDRTB, maintaining isolation throughout hospitalization is prudent [1].
Discharge planning Cooperation between hospital staff and the local public health department is essential. Discharge to home may be considered once the following conditions are met: An outpatient appointment has been arranged with a provider who will manage TB Case management from the local public health department is involved and agrees with the plan The patient is in possession of sufficient anti-TB medication (not just the prescriptions) to last until the outpatient appointment A patient may be discharged to home while still infectious, provided that the household does not contain members at high risk for active TB (eg, immunocompromised or age less than four) [1]. While still considered infectious, the patient should stay home as much as possible and should wear a surgical mask when leaving the home or when receiving visitors. Outpatient management Many persons with active TB will first present to an ambulatory care site. Patients who may have active TB must be identified and evaluated promptly in order to minimize exposure of others. Ideally, such patients should be placed in an AII room; if unavailable, an enclosed area should be used and a surgical mask (not an N95 mask) should be placed on the patient [1]. The patient should be instructed to cover the mouth and nose with tissues when sneezing or coughing. If an area other than an AII room is used, it should not be used again for one hour once the patient has left. Once a patient is diagnosed with active TB, such precautions should continue until the patient is deemed noninfectious. Whenever possible, appointments for known TB cases should be scheduled to avoid contact with immunocompromised patients, such as persons with HIV.
Ambulatory care sites that treat a high volume of patients with TB or at high risk for TB should consider having at least one AII room and should consider enhancing general ventilation and/or using air disinfection techniques such as ultraviolet germicidal irradiation, and/or high efficiency particulate air (HEPA) filters [1]. CONTACT INVESTIGATION A contact investigation should be initiated to promptly identify secondary cases of active and latent TB in the following circumstances [1]: Evaluation of a patient with active TB in a healthcare setting without prompt institution of infection control measures Identification of active TB in a healthcare worker with exposure to others in the healthcare setting The investigation should proceed in collaboration with the local or state public health department. The index case should be interviewed and his or her medical records reviewed. An individual with AFB smear-positive involving the respiratory tract is generally considered to have been contagious starting three months before the first smear-positive sputum or onset of pertinent symptoms, whichever is earlier. For persons with AFB smear-negative disease, the contagious period is considered to have begun one month before the onset of symptoms. The contagious period is considered to end with the institution of airborne precautions [1]. HCWs and patients with potential exposure should be screened (by symptoms and, unless positive at baseline, TST or IGRA) as soon as possible after the exposure. If initial screening is negative testing should be repeated 8 to 10 weeks following the end of the exposure. Identification of individuals with LTBI or active disease should prompt expansion of the investigation to include individuals with less intense contact with the index patient [1].
Exposed persons with HIV infection should be evaluated for the initiation of preventive therapy once active disease has been ruled out, regardless of TST or IGRA results [23]. Family members and other close contacts of index cases of active TB also need to be assessed. Identification of healthcare-associated tuberculin test conversion should prompt review of institutional TB control policy and practices [1].
13.
14.
15.
16.
REFERENCES 1. Centers for Disease Control and Prevention (CDC). Health disparities experienced by black or African Americans--United States. MMWR Morb Mortal Wkly Rep 2005; 54:1. Sepkowitz KA. How contagious is tuberculosis? Clin Infect Dis 1996; 23:954. Loudon RG, Spohn SK. Cough frequency and infectivity in patients with pulmonary tuberculosis. Am Rev Respir Dis 1969; 99:109. Loudon RG, Roberts RM. Droplet expulsion from the respiratory tract. Am Rev Respir Dis 1967; 95:435. Loudon RG, Roberts RM. Singing and the dissemination of tuberculosis. Am Rev Respir Dis 1968; 98:297. BATES JH, POTTS WE, LEWIS M. EPIDEMIOLOGY OF PRIMARY TUBERCULOSIS IN AN INDUSTRIAL SCHOOL. N Engl J Med 1965; 272:714. Tostmann A, Kik SV, Kalisvaart NA, et al. Tuberculosis transmission by patients with smear-negative pulmonary tuberculosis in a large cohort in the Netherlands. Clin Infect Dis 2008; 47:1135. Edlin BR, Tokars JI, Grieco MH, et al. An outbreak of multidrug-resistant tuberculosis among hospitalized patients with the acquired immunodeficiency syndrome. N Engl J Med 1992; 326:1514. Beck-Sagu C, Dooley SW, Hutton MD, et al. Hospital outbreak of multidrug-resistant Mycobacterium tuberculosis infections. Factors in transmission to staff and HIV-infected patients. JAMA 1992; 268:1280. Centers for Disease Control (CDC). Nosocomial transmission of multidrugresistant tuberculosis to health-care workers and HIV-infected patients in an urban hospital--Florida. MMWR Morb Mortal Wkly Rep 1990; 39:718. Centers for Disease Control (CDC). Nosocomial transmission of multidrugresistant tuberculosis among HIV-infected persons--Florida and New York, 19881991. MMWR Morb Mortal Wkly Rep 1991; 40:585. Pearson ML, Jereb JA, Frieden TR, et al. Nosocomial transmission of multidrug-resistant Mycobacterium tuberculosis. A risk to patients and health care workers. Ann Intern Med 1992; 117:191.
17.
18.
2. 3. 4. 5. 6. 7.
19.
20.
21.
8.
22.
9.
23.
Centers for Disease Control (CDC). Tuberculosis outbreak among persons in a residential facility for HIV-infected persons--San Francisco. MMWR Morb Mortal Wkly Rep 1991; 40:649. Daley CL, Small PM, Schecter GF, et al. An outbreak of tuberculosis with accelerated progression among persons infected with the human immunodeficiency virus. An analysis using restriction-fragment-length polymorphisms. N Engl J Med 1992; 326:231. Frieden TR, Sherman LF, Maw KL, et al. A multi-institutional outbreak of highly drug-resistant tuberculosis: epidemiology and clinical outcomes. JAMA 1996; 276:1229. Larsen NM, Biddle CL, Sotir MJ, et al. Risk of tuberculin skin test conversion among health care workers: occupational versus community exposure and infection. Clin Infect Dis 2002; 35:796. Moran GJ, Barrett TW, Mower WR, et al. Decision instrument for the isolation of pneumonia patients with suspected pulmonary tuberculosis admitted through US emergency departments. Ann Emerg Med 2009; 53:625. Perlman DC, el-Sadr WM, Nelson ET, et al. Variation of chest radiographic patterns in pulmonary tuberculosis by degree of human immunodeficiency virusrelated immunosuppression. The Terry Beirn Community Programs for Clinical Research on AIDS (CPCRA). The AIDS Clinical Trials Group (ACTG). Clin Infect Dis 1997; 25:242. Peterson EM, Nakasone A, Platon-DeLeon JM, et al. Comparison of direct and concentrated acid-fast smears to identify specimens culture positive for Mycobacterium spp. J Clin Microbiol 1999; 37:3564. Tokars JI, McKinley GF, Otten J, et al. Use and efficacy of tuberculosis infection control practices at hospitals with previous outbreaks of multidrug-resistant tuberculosis. Infect Control Hosp Epidemiol 2001; 22:449. Sutton PM, Nicas M, Harrison RJ. Tuberculosis isolation: comparison of written procedures and actual practices in three California hospitals. Infect Control Hosp Epidemiol 2000; 21:28. Noble, RC. Infectiousness of pulmonary tuberculosis after starting chemotherapy: review of the available data on an unresolved question. Am J Infect Control 1981; 9:6. CDC. Prevention and treatment of tuberculosis among patients infected with human immunodeficiency virus: Principles of therapy and revised recommendations. MMWR 1998; 47(RR-20).
10.
11.
12.
Das könnte Ihnen auch gefallen
- Journal Pone 0035292Dokument9 SeitenJournal Pone 0035292Amrina RosyadaNoch keine Bewertungen
- Contibutors For CI 1852Dokument6 SeitenContibutors For CI 1852Amrina RosyadaNoch keine Bewertungen
- Puku L TD Nadi RR Suhu Spo2 IntervensiDokument1 SeitePuku L TD Nadi RR Suhu Spo2 IntervensiAmrina RosyadaNoch keine Bewertungen
- Thomas Jacobson 2010Dokument23 SeitenThomas Jacobson 2010Amrina RosyadaNoch keine Bewertungen
- (Blok 23) - Distribusi Soal MCQ Hari Ke-1 Dan Ke-2Dokument2 Seiten(Blok 23) - Distribusi Soal MCQ Hari Ke-1 Dan Ke-2Amrina RosyadaNoch keine Bewertungen
- 07 044503Dokument8 Seiten07 044503Amrina RosyadaNoch keine Bewertungen
- Obstetricia - Abnormal Uterine Bleeding DefinitionsDokument2 SeitenObstetricia - Abnormal Uterine Bleeding DefinitionsJadder InnacioNoch keine Bewertungen
- Thomas Jacobson 2010Dokument23 SeitenThomas Jacobson 2010Amrina RosyadaNoch keine Bewertungen
- En 16Dokument38 SeitenEn 16Sonia RogersNoch keine Bewertungen
- Presentation TitleDokument2 SeitenPresentation Titleriena456Noch keine Bewertungen
- Jaas 3 1 09LDokument5 SeitenJaas 3 1 09LAmrina RosyadaNoch keine Bewertungen
- Diagnosis WorksheetDokument2 SeitenDiagnosis Worksheetnurul ramadhanyNoch keine Bewertungen
- Antibiotic Endometritis CochraneDokument56 SeitenAntibiotic Endometritis CochraneAmrina RosyadaNoch keine Bewertungen
- 2011 CAP in ChildrenDokument52 Seiten2011 CAP in Childrenbebekdd22Noch keine Bewertungen
- Critical Care Therapy and Respiratory Care SectionDokument12 SeitenCritical Care Therapy and Respiratory Care SectionPhysio EbookNoch keine Bewertungen
- Journal Pmed 0030276Dokument4 SeitenJournal Pmed 0030276Amrina RosyadaNoch keine Bewertungen
- Diagnosis WorksheetDokument2 SeitenDiagnosis Worksheetnurul ramadhanyNoch keine Bewertungen
- Pre EclampsiaDokument2 SeitenPre EclampsiaAmrina RosyadaNoch keine Bewertungen
- Diagnosis WorksheetDokument2 SeitenDiagnosis Worksheetnurul ramadhanyNoch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Series Screenwriter Portfolio by SlidesgoDokument24 SeitenSeries Screenwriter Portfolio by SlidesgoYeddah Gwyneth TiuNoch keine Bewertungen
- International Journal of EpidemiologyDokument9 SeitenInternational Journal of Epidemiologycooky maknaeNoch keine Bewertungen
- Infection ControlDokument3 SeitenInfection ControlHazelina VillamorNoch keine Bewertungen
- 2019 Externship Survey 07242019 FINALDokument494 Seiten2019 Externship Survey 07242019 FINALddNoch keine Bewertungen
- Aerobic Dancing BenefitsDokument4 SeitenAerobic Dancing BenefitsDal.giNoch keine Bewertungen
- Diagnosis and Management of Diabetic Foot ComplicaDokument25 SeitenDiagnosis and Management of Diabetic Foot Complicafebyan yohanesNoch keine Bewertungen
- Barodontalgia 2009Dokument6 SeitenBarodontalgia 2009Maganti Sai SandeepNoch keine Bewertungen
- Ayurveda Association of Singapore SWOT AnalysisDokument15 SeitenAyurveda Association of Singapore SWOT AnalysisOng Saviour NicholasNoch keine Bewertungen
- The Hall Technique: Food for ThoughtDokument50 SeitenThe Hall Technique: Food for ThoughtMustafa Tambawala100% (1)
- (IU-GADSOP 2018) (A4) First Announcement - Versi ADokument1 Seite(IU-GADSOP 2018) (A4) First Announcement - Versi AIfah Inayah D'zatrichaNoch keine Bewertungen
- Single Denture - II-Combination SyndromeDokument30 SeitenSingle Denture - II-Combination SyndromeIsmail HamadaNoch keine Bewertungen
- NCPDokument2 SeitenNCPsphinx809100% (2)
- Nursing FoundationDokument48 SeitenNursing Foundationgayathri rayapudiNoch keine Bewertungen
- PATHFit 1 Module 1 1Dokument9 SeitenPATHFit 1 Module 1 1Danielle Jhon Tevdcian OmegaNoch keine Bewertungen
- Glycemic Targets 2022Dokument14 SeitenGlycemic Targets 2022Tom BiusoNoch keine Bewertungen
- MTLB Debate PRODokument3 SeitenMTLB Debate PRORHODA MAE CAPUTOLNoch keine Bewertungen
- Clinical Practice Guidelines for Hepatitis B Virus (HBV) ManagementDokument48 SeitenClinical Practice Guidelines for Hepatitis B Virus (HBV) ManagementAqila MumtazNoch keine Bewertungen
- Japan Metabo LawDokument16 SeitenJapan Metabo LawReginNoch keine Bewertungen
- StiDokument12 SeitenStiValentinaNoch keine Bewertungen
- B.SC NURSING SubjectWiseDokument105 SeitenB.SC NURSING SubjectWiseGeorge9688Noch keine Bewertungen
- SalesDokument2 SeitenSalesapi-77262028Noch keine Bewertungen
- A Cross Sectional Survey On Sleep Quality, Mental Health, and Academic Performance Among Medical Student in Saudia ArabiaDokument5 SeitenA Cross Sectional Survey On Sleep Quality, Mental Health, and Academic Performance Among Medical Student in Saudia ArabiaReynaldy Anggara SaputraNoch keine Bewertungen
- Closing Event For Surrey Perinatal Impact PartnershipDokument11 SeitenClosing Event For Surrey Perinatal Impact Partnershipranjanadas0% (1)
- Epiglottitis and LaryngitisDokument9 SeitenEpiglottitis and Laryngitisputri balqisNoch keine Bewertungen
- Antibiotic StewardshipDokument6 SeitenAntibiotic Stewardshipkyliever100% (1)
- Legal and Ethical Issues in NursingDokument53 SeitenLegal and Ethical Issues in Nursingkrishnasree100% (2)
- Sanction Terms Loan DetailsDokument4 SeitenSanction Terms Loan Detailsinfoski khan100% (1)
- Student's Handbook 2014Dokument52 SeitenStudent's Handbook 2014Ahmed MawahibNoch keine Bewertungen
- Contingency Plan For Covid 19Dokument27 SeitenContingency Plan For Covid 19Oteee17Noch keine Bewertungen
- INTL ARRIVALSDokument9 SeitenINTL ARRIVALSKoushik SekharNoch keine Bewertungen