Das könnte Ihnen auch gefallen
- Tracker December 01 To 12TH 2020Dokument12 SeitenTracker December 01 To 12TH 2020Nasir AhmedNoch keine Bewertungen
- PhySICS Paper With AnswerDokument5 SeitenPhySICS Paper With Answersudhir_narang_3Noch keine Bewertungen
- Abhi18 PDFDokument8 SeitenAbhi18 PDFNasir AhmedNoch keine Bewertungen
- Abhi18 PDFDokument8 SeitenAbhi18 PDFNasir AhmedNoch keine Bewertungen
- FMCG ChaneelDokument4 SeitenFMCG ChaneelNasir AhmedNoch keine Bewertungen
- Neet Code A Question PaperDokument41 SeitenNeet Code A Question PaperRohit Kumar JenaNoch keine Bewertungen
- Quotation For Light WeightDokument2 SeitenQuotation For Light WeightNasir AhmedNoch keine Bewertungen
- Loan To Non Member BranchID Dump1001Dokument250 SeitenLoan To Non Member BranchID Dump1001Nasir AhmedNoch keine Bewertungen
- Details of Verified Recruiting AgenciesDokument90 SeitenDetails of Verified Recruiting AgenciesNasir AhmedNoch keine Bewertungen
- Arabian Consultants Pvt. LTDDokument6 SeitenArabian Consultants Pvt. LTDNasir AhmedNoch keine Bewertungen
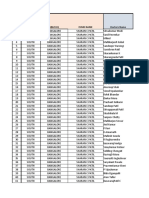
- Appointment TableDokument6 SeitenAppointment TableNasir AhmedNoch keine Bewertungen
- Allen: Neet-2017 Test Paper With Answer & Solutions (Held On Sunday 07 MAY, 2017)Dokument7 SeitenAllen: Neet-2017 Test Paper With Answer & Solutions (Held On Sunday 07 MAY, 2017)Anurag LaddhaNoch keine Bewertungen
- VCS BrochureDokument13 SeitenVCS BrochureNasir AhmedNoch keine Bewertungen
- Business Models, Business Strategy and InnovationDokument23 SeitenBusiness Models, Business Strategy and InnovationTran Quoc Dong100% (3)
- Dam Maya Magar 509 Sumita Tamang: Hamsa Kalathil Valappil Muhammed Kalathil Valappil Siddique MuhammedDokument1 SeiteDam Maya Magar 509 Sumita Tamang: Hamsa Kalathil Valappil Muhammed Kalathil Valappil Siddique MuhammedNasir AhmedNoch keine Bewertungen
- Shortcut Key For WindowsDokument2 SeitenShortcut Key For WindowsNasir AhmedNoch keine Bewertungen
- AF21417 - Business Development Manager - Open Day Recruitment - Orient - UAEDokument14 SeitenAF21417 - Business Development Manager - Open Day Recruitment - Orient - UAENasir AhmedNoch keine Bewertungen
- Joel AbrahamDokument5 SeitenJoel AbrahamNasir AhmedNoch keine Bewertungen
- New Microsoft Word 97 - 2003 DocumentDokument1 SeiteNew Microsoft Word 97 - 2003 DocumentNasir AhmedNoch keine Bewertungen
- PracticeDokument12 SeitenPracticeNasir AhmedNoch keine Bewertungen
- Social Science EngMQP - 2Dokument4 SeitenSocial Science EngMQP - 2Nasir AhmedNoch keine Bewertungen
- Back Page 2Dokument1 SeiteBack Page 2Nasir AhmedNoch keine Bewertungen
- Á Àä Æã/ Æ Gádpàä Àiágà Vàazé À Àgád ºàauàgàv, Àaiàä Àäì: - Gzéæåãuà: Àå Àºágà Á: C Àgázà (©) Vá.F. Uàä® Uáð Àiáqàä À Àæ Àiát Àvàæ J ÉazàgéDokument1 SeiteÁ Àä Æã/ Æ Gádpàä Àiágà Vàazé À Àgád ºàauàgàv, Àaiàä Àäì: - Gzéæåãuà: Àå Àºágà Á: C Àgázà (©) Vá.F. Uàä® Uáð Àiáqàä À Àæ Àiát Àvàæ J ÉazàgéNasir AhmedNoch keine Bewertungen
- The Following Detailed of The Product Specification: Civil Engineering Grade BentoniteDokument2 SeitenThe Following Detailed of The Product Specification: Civil Engineering Grade BentoniteNasir AhmedNoch keine Bewertungen
- Online Application For Gazetted Probationers Preliminary Examination - 2014Dokument2 SeitenOnline Application For Gazetted Probationers Preliminary Examination - 2014Nasir AhmedNoch keine Bewertungen
- Civil Engineering Grade BentoniteDokument1 SeiteCivil Engineering Grade BentoniteNasir AhmedNoch keine Bewertungen
- Online Application For Gazetted Probationers Preliminary Examination - 2014Dokument2 SeitenOnline Application For Gazetted Probationers Preliminary Examination - 2014Nasir AhmedNoch keine Bewertungen
- Income and Caste Certificate: Government of Karnataka Revenue Derpartmet Form-F Gulbarga TalukDokument2 SeitenIncome and Caste Certificate: Government of Karnataka Revenue Derpartmet Form-F Gulbarga TalukNasir AhmedNoch keine Bewertungen
- House For RentDokument1 SeiteHouse For RentNasir AhmedNoch keine Bewertungen
- IEC OnlineDokument37 SeitenIEC OnlinespotdealNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Kumari Mitakshara 70865394 India Vocational Education TrainingDokument27 SeitenKumari Mitakshara 70865394 India Vocational Education TrainingManoj PendyalaNoch keine Bewertungen
- Important Qualities of A Good SupervisorDokument3 SeitenImportant Qualities of A Good SupervisorzamiltonNoch keine Bewertungen
- Model Recruitment Contract Annex C V Aug14Dokument4 SeitenModel Recruitment Contract Annex C V Aug14api-258233781Noch keine Bewertungen
- A Study On Grivence Management in Improving Employees in A Privete EnterpriseDokument52 SeitenA Study On Grivence Management in Improving Employees in A Privete Enterpriseavinash bulusuNoch keine Bewertungen
- NSNP 200 Employer Information EnglishDokument12 SeitenNSNP 200 Employer Information EnglishMotivational speaker Pratham GuptaNoch keine Bewertungen
- Pplication ORM: Ersonal EtailsDokument5 SeitenPplication ORM: Ersonal EtailsAnaz KalliyathNoch keine Bewertungen
- 4 McDonald Hernandez McDonald Et Al ERRJ 2008Dokument8 Seiten4 McDonald Hernandez McDonald Et Al ERRJ 2008Tengiz VerulavaNoch keine Bewertungen
- Electrical Arcing Phenomena Based On IEEE 1584 & NFPA 70EDokument11 SeitenElectrical Arcing Phenomena Based On IEEE 1584 & NFPA 70Ekspm007100% (1)
- Time Book and PayrollDokument9 SeitenTime Book and PayrollStefano Abao OyanNoch keine Bewertungen
- Codependency Workplace PP TDokument36 SeitenCodependency Workplace PP TPipatico100% (2)
- 4th S-ToPIK List of PassersDokument6 Seiten4th S-ToPIK List of PassersEli Benjamin Nava TaclinoNoch keine Bewertungen
- Utrecht ScaleDokument58 SeitenUtrecht ScaleMaya CamarasuNoch keine Bewertungen
- Confidence and Competence, Their Relationship and Impact On Workplace PerformanceDokument87 SeitenConfidence and Competence, Their Relationship and Impact On Workplace PerformanceJules Savage-MilnerNoch keine Bewertungen
- Labor Law (Authorized Causes) DigestsDokument28 SeitenLabor Law (Authorized Causes) Digestsanna bee100% (2)
- Labour ORdinance SabahDokument89 SeitenLabour ORdinance SabahApeng Bah IniNoch keine Bewertungen
- Villa V NLRCDokument3 SeitenVilla V NLRCJackie Canlas100% (1)
- Inc Tnai IcnDokument7 SeitenInc Tnai IcnDeena MelvinNoch keine Bewertungen
- Chapter 4Dokument39 SeitenChapter 4sofikhdy100% (1)
- Vicarious LiabilityDokument5 SeitenVicarious Liabilitykeshni_sritharanNoch keine Bewertungen
- Topic 7 - Workplace Basic Issues (Week5)Dokument10 SeitenTopic 7 - Workplace Basic Issues (Week5)Pei JuanNoch keine Bewertungen
- Term Paper - Labour & Industrial LawDokument19 SeitenTerm Paper - Labour & Industrial LawSOGIR AHMAD100% (1)
- Aditya Raj - CA 4 - HM-EE-401Dokument15 SeitenAditya Raj - CA 4 - HM-EE-401sajid0khan-790945Noch keine Bewertungen
- Checklist of Requirements - Job Order (Landbased) For POLO OWWADokument1 SeiteChecklist of Requirements - Job Order (Landbased) For POLO OWWAMaybelNoch keine Bewertungen
- Organisation ChangeDokument15 SeitenOrganisation ChangeAssignmentLab.com100% (1)
- (Advanced Academic Research Activity) Point Calculation Table For Highly Skilled Professional (I) (A) & (Ii)Dokument24 Seiten(Advanced Academic Research Activity) Point Calculation Table For Highly Skilled Professional (I) (A) & (Ii)roettgersNoch keine Bewertungen
- OT Practice Exercise-1Dokument3 SeitenOT Practice Exercise-1Savita Choudhary0% (1)
- Mpy315 FinalDokument21 SeitenMpy315 FinalCharles ChivengahNoch keine Bewertungen
- Fti Tvet Leadership & Management: Course: Tvet Management By: Bekre H. (PHD) Addis Ababa EthiopiaDokument113 SeitenFti Tvet Leadership & Management: Course: Tvet Management By: Bekre H. (PHD) Addis Ababa EthiopiaTsega BirhanuNoch keine Bewertungen
- Apprenticeship Program Agreement and Liability Waiver-1Dokument2 SeitenApprenticeship Program Agreement and Liability Waiver-1James Dela Cruz100% (2)
- UntitledDokument110 SeitenUntitledtrang huyềnNoch keine Bewertungen