Das könnte Ihnen auch gefallen
- ICU Scoring Systems A Complete Guide - 2020 EditionVon EverandICU Scoring Systems A Complete Guide - 2020 EditionNoch keine Bewertungen
- Advanced Airway Care: Intensive Care Unit PerspectiveDokument42 SeitenAdvanced Airway Care: Intensive Care Unit PerspectiveJeffery Samuel100% (1)
- Drugs in Cardiac EnmergenciesDokument94 SeitenDrugs in Cardiac EnmergenciesVijayan VelayudhanNoch keine Bewertungen
- Pediatric Assessment: General ImpressionDokument2 SeitenPediatric Assessment: General ImpressionAghnia Nafila100% (1)
- Adult Infusion StandardsDokument11 SeitenAdult Infusion StandardsJessica Torreglosa100% (1)
- Acccn Paed Interactive Manual 2018Dokument108 SeitenAcccn Paed Interactive Manual 2018Seb KirbyNoch keine Bewertungen
- Emergency Department Intubation ChecklisTDokument2 SeitenEmergency Department Intubation ChecklisTStacey Woods100% (1)
- Continuous Quality Improvement IndicatorsDokument10 SeitenContinuous Quality Improvement Indicatorsaaminah tariq100% (1)
- Acls Course HandoutsDokument8 SeitenAcls Course HandoutsRoxas CedrickNoch keine Bewertungen
- Care of Patient With TPM Slide PresentationDokument16 SeitenCare of Patient With TPM Slide PresentationirzehronNoch keine Bewertungen
- 2017 05 GC Pocket CardDokument2 Seiten2017 05 GC Pocket Cardapi-312241089Noch keine Bewertungen
- ICU One Pager EVD V11Dokument1 SeiteICU One Pager EVD V11Mohamed Mahmoud100% (1)
- Neurological Examination PDFDokument6 SeitenNeurological Examination PDFArif K BashaNoch keine Bewertungen
- Kdoqi Vasc Access Review2019 v2Dokument163 SeitenKdoqi Vasc Access Review2019 v2Humairah AnandaNoch keine Bewertungen
- Angina Pharmacology YeahDokument16 SeitenAngina Pharmacology YeahMuhammad AfifuddinNoch keine Bewertungen
- Nursing Responsibilities For The Patient Will Undergo Cardiac CatheterizationDokument4 SeitenNursing Responsibilities For The Patient Will Undergo Cardiac CatheterizationCharlene Jacobe Cornista100% (1)
- Anesthesiology Pre-Op Evaluation: ExovsrtsDokument1 SeiteAnesthesiology Pre-Op Evaluation: Exovsrtssabbo morsNoch keine Bewertungen
- Airway and The NurseDokument7 SeitenAirway and The NursecarmenbuleandraNoch keine Bewertungen
- CRITICAL CARE, March 2020Dokument47 SeitenCRITICAL CARE, March 2020Jonathan Yeoh100% (1)
- Abcde ApproachDokument3 SeitenAbcde ApproachMaria Isabel Medina MesaNoch keine Bewertungen
- CCU Clinical GuidelinesDokument63 SeitenCCU Clinical GuidelinesHAMMYER ALROKHAMINoch keine Bewertungen
- Sedation in The IcuDokument4 SeitenSedation in The Icuprashsubbu100% (1)
- Chest Pain: Jean J. Chatham, MDDokument40 SeitenChest Pain: Jean J. Chatham, MDYermia RashaquatNoch keine Bewertungen
- CCUDokument82 SeitenCCUSarah100% (1)
- HW InotropesDokument3 SeitenHW InotropesNatalie YeohNoch keine Bewertungen
- Acute Stroke Nursing GuidelineFINAL 1 2Dokument5 SeitenAcute Stroke Nursing GuidelineFINAL 1 2radanikmaNoch keine Bewertungen
- Definitions: Transfusion Reactions:: 2,3-BPG Is Degraded in StorageDokument1 SeiteDefinitions: Transfusion Reactions:: 2,3-BPG Is Degraded in Storagejuan ramon milanes grageraNoch keine Bewertungen
- ECMO and Right Ventricular FailureDokument9 SeitenECMO and Right Ventricular FailureLuis Fernando Morales JuradoNoch keine Bewertungen
- Arterial Lines in PACU: Presented by Autum Jacobs RN, BSNDokument34 SeitenArterial Lines in PACU: Presented by Autum Jacobs RN, BSNinuko1212Noch keine Bewertungen
- Basic Mechanical Ventilation 2014Dokument62 SeitenBasic Mechanical Ventilation 2014dragon66Noch keine Bewertungen
- Agenda Bls-AclsDokument2 SeitenAgenda Bls-AclsespegehNoch keine Bewertungen
- Using The ACLS Primary Survey For A Patient in Respiratory ArrestDokument34 SeitenUsing The ACLS Primary Survey For A Patient in Respiratory Arrest강기연100% (1)
- DPN Icu PDFDokument1 SeiteDPN Icu PDFharoonNoch keine Bewertungen
- Standard Treatment WorkflowsDokument75 SeitenStandard Treatment WorkflowsIndranil DuttaNoch keine Bewertungen
- Presentation Q06 Certified ProfeDokument304 SeitenPresentation Q06 Certified ProfeMemo MedoNoch keine Bewertungen
- Critical Care SedationVon EverandCritical Care SedationAngelo Raffaele De GaudioNoch keine Bewertungen
- Tracheostomy Guidelines 2018Dokument97 SeitenTracheostomy Guidelines 2018KateCuadraNoch keine Bewertungen
- Vasoactive Agents For Adult Septic Shock: An Update and ReviewDokument10 SeitenVasoactive Agents For Adult Septic Shock: An Update and ReviewntnquynhproNoch keine Bewertungen
- Pre-Op Assessment: Dr. Ayesha Ehsan House Surgeon S-IIDokument25 SeitenPre-Op Assessment: Dr. Ayesha Ehsan House Surgeon S-IIFatima MNoch keine Bewertungen
- A Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsVon EverandA Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsNoch keine Bewertungen
- Management of Arterial LineDokument16 SeitenManagement of Arterial LineFarcasanu Liana GeorgianaNoch keine Bewertungen
- Complications of Blood TransfusionsDokument4 SeitenComplications of Blood TransfusionsZain Hadi100% (1)
- Jcinabhqualityimprovementproposal1 150301235729 Conversion Gate02Dokument31 SeitenJcinabhqualityimprovementproposal1 150301235729 Conversion Gate02Abhishek TrivediNoch keine Bewertungen
- Module 9 Mechanical Ventilation PDFDokument46 SeitenModule 9 Mechanical Ventilation PDFChabboo SutabrataNoch keine Bewertungen
- Evidence Based Nursing PracticeDokument21 SeitenEvidence Based Nursing Practiceshenric16Noch keine Bewertungen
- How To Treat: Septic ShockDokument6 SeitenHow To Treat: Septic ShockmeeandsoeNoch keine Bewertungen
- Cs-Cardiac-023-Essential Cardiac LabsDokument2 SeitenCs-Cardiac-023-Essential Cardiac LabsColeen YraolaNoch keine Bewertungen
- RFDS Western Operations HEA16 - V3.0 Clinical ManualDokument28 SeitenRFDS Western Operations HEA16 - V3.0 Clinical ManualJoed BiasonNoch keine Bewertungen
- Icu Sop: TOPIC: Length of Stay in ICUDokument5 SeitenIcu Sop: TOPIC: Length of Stay in ICURohit RajeevanNoch keine Bewertungen
- Practice Standards For The Emergency Nurse Specialist. CENA, 2014Dokument16 SeitenPractice Standards For The Emergency Nurse Specialist. CENA, 2014Cristobal Alejandro Falado SantanderNoch keine Bewertungen
- Procedural Sedation - Audit Information 2017-18Dokument14 SeitenProcedural Sedation - Audit Information 2017-18Anonymous msnwfNd0% (1)
- Fluid and Electrolyte Balance in ICUDokument46 SeitenFluid and Electrolyte Balance in ICUtapas_kbNoch keine Bewertungen
- Shock Study GuideDokument8 SeitenShock Study GuideMadameb1Noch keine Bewertungen
- Walhalla Gold MineDokument1 SeiteWalhalla Gold MineYwagar YwagarNoch keine Bewertungen
- Clinical Tutorial 2008.11.05Dokument31 SeitenClinical Tutorial 2008.11.05Ywagar Ywagar100% (1)
- Sydney 2008 MarchDokument8 SeitenSydney 2008 MarchYwagar YwagarNoch keine Bewertungen
- Recall Brisbane February 2008Dokument7 SeitenRecall Brisbane February 2008Ywagar YwagarNoch keine Bewertungen
- Clinical Recall 17 May 2008 Melbourne: AMC Feedback: Sudden Infant Death SyndromeDokument14 SeitenClinical Recall 17 May 2008 Melbourne: AMC Feedback: Sudden Infant Death SyndromeYwagar YwagarNoch keine Bewertungen
- Adelaide, 5 April, 2008: PaediatricsDokument17 SeitenAdelaide, 5 April, 2008: PaediatricsYwagar YwagarNoch keine Bewertungen
- Brisbane July 2008 RecallDokument11 SeitenBrisbane July 2008 RecallYwagar YwagarNoch keine Bewertungen
- GPDokument3 SeitenGPYwagar YwagarNoch keine Bewertungen
- Draft May 08 WES ProgramDokument2 SeitenDraft May 08 WES ProgramYwagar YwagarNoch keine Bewertungen
- Adelaide 13th September 2008Dokument16 SeitenAdelaide 13th September 2008Ywagar YwagarNoch keine Bewertungen
- Adelaide, 5 April, 2008: PaediatricsDokument17 SeitenAdelaide, 5 April, 2008: PaediatricsYwagar YwagarNoch keine Bewertungen
- BrisDokument9 SeitenBrisYwagar YwagarNoch keine Bewertungen
- ACln2007!09!08MEL Retest Wd97Dokument6 SeitenACln2007!09!08MEL Retest Wd97Ywagar YwagarNoch keine Bewertungen
- Melbourne 2008 Nov 8Dokument10 SeitenMelbourne 2008 Nov 8Ywagar YwagarNoch keine Bewertungen
- Melb RetestDokument4 SeitenMelb RetestYwagar YwagarNoch keine Bewertungen
- Paediatrics:: Case 1nsionDokument16 SeitenPaediatrics:: Case 1nsionYwagar YwagarNoch keine Bewertungen
- Brisbane, 11th October 2008Dokument6 SeitenBrisbane, 11th October 2008Ywagar YwagarNoch keine Bewertungen
- Clinical Recall 17 May 2008 Melbourne: AMC Feedback: Sudden Infant Death SyndromeDokument14 SeitenClinical Recall 17 May 2008 Melbourne: AMC Feedback: Sudden Infant Death SyndromeYwagar YwagarNoch keine Bewertungen
- Melbourne, 9 February 2008: AMC Feedback: Paranoid Schizophrenia (Relapse)Dokument13 SeitenMelbourne, 9 February 2008: AMC Feedback: Paranoid Schizophrenia (Relapse)Ywagar YwagarNoch keine Bewertungen
- Brisbane February 2008: Peanut Induced AnaphylaxisDokument7 SeitenBrisbane February 2008: Peanut Induced AnaphylaxisYwagar YwagarNoch keine Bewertungen
- 15th March 2008 SydneyDokument3 Seiten15th March 2008 SydneyYwagar YwagarNoch keine Bewertungen
- 3rd May 2008 SydneyDokument9 Seiten3rd May 2008 SydneyYwagar YwagarNoch keine Bewertungen
- Proposal QUAL MoralesDokument101 SeitenProposal QUAL MoralesFrederick BaldemoroNoch keine Bewertungen
- ThesisDokument64 SeitenThesisiojnilnjkhNoch keine Bewertungen
- Claims Management and Substantiation in The United Arab Emirates Construction SectorDokument123 SeitenClaims Management and Substantiation in The United Arab Emirates Construction SectorFIDICglykysNoch keine Bewertungen
- Science 7 Scientific Methods Week 1Dokument3 SeitenScience 7 Scientific Methods Week 1Samina ManasNoch keine Bewertungen
- ENGR 101 Quiz 1 Section 2457 SolutionsDokument2 SeitenENGR 101 Quiz 1 Section 2457 SolutionsalishehadehNoch keine Bewertungen
- Specifications Indoor-Air-comfort v6 enDokument25 SeitenSpecifications Indoor-Air-comfort v6 enelezmNoch keine Bewertungen
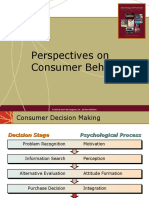
- Perspectives On Consumer Behavior: © 2003 Mcgraw-Hill Companies, Inc., Mcgraw-Hill/IrwinDokument28 SeitenPerspectives On Consumer Behavior: © 2003 Mcgraw-Hill Companies, Inc., Mcgraw-Hill/IrwinUMAR KHANNoch keine Bewertungen
- Mergers and Acquisitions - The Four (4) Greatest Risk Factors For Leaders and ManagersDokument6 SeitenMergers and Acquisitions - The Four (4) Greatest Risk Factors For Leaders and ManagersZenn Maia GuerreroNoch keine Bewertungen
- Group Assignment 2: SB2023 Dr. Le Anh TuanDokument2 SeitenGroup Assignment 2: SB2023 Dr. Le Anh TuanHuyen cao thi thanhNoch keine Bewertungen
- Chapter 3. Sales & Operations Aggregate) PlanningDokument47 SeitenChapter 3. Sales & Operations Aggregate) PlanningsanjaykhatwaniNoch keine Bewertungen
- Strut and Tie Modelling of Reinforced Concrete DeepDokument18 SeitenStrut and Tie Modelling of Reinforced Concrete DeepHunny VermaNoch keine Bewertungen
- IS481GSSR ProcessSimulationDokument17 SeitenIS481GSSR ProcessSimulationalhanoofalsagirNoch keine Bewertungen
- Difference Between Thesis and Dissertation UkDokument7 SeitenDifference Between Thesis and Dissertation Ukaflpbevnrabaqk100% (2)
- OrganizingDokument46 SeitenOrganizingViswajeet BiswalNoch keine Bewertungen
- The Secretary and The Effect of New Office Technologies On Record Keeping ManagementDokument12 SeitenThe Secretary and The Effect of New Office Technologies On Record Keeping ManagementMorenikeji Adewale33% (3)
- Annotated Reference ListDokument2 SeitenAnnotated Reference Listapi-240839049Noch keine Bewertungen
- Toothpaste Survey (2021)Dokument20 SeitenToothpaste Survey (2021)Aashish KuNoch keine Bewertungen
- Studies Guide IGCSEDokument15 SeitenStudies Guide IGCSESamar Hamady100% (1)
- Semester Reflections 1Dokument3 SeitenSemester Reflections 1api-457886715Noch keine Bewertungen
- Technical Communication Unit 1Dokument15 SeitenTechnical Communication Unit 1Sandhya RNoch keine Bewertungen
- Warren (2011) Sistematic ReviewDokument11 SeitenWarren (2011) Sistematic ReviewMariaClaradeFreitasNoch keine Bewertungen
- Presentation StrategyDokument40 SeitenPresentation StrategyAbdullah ghauriNoch keine Bewertungen
- Hypothesis Statement and Statistical Testing: A TutorialDokument7 SeitenHypothesis Statement and Statistical Testing: A TutorialBOHR International Journal of Operations Management Research and Practices (BIJOMRP)Noch keine Bewertungen
- Kindly Reply With Following Details:: TH THDokument2 SeitenKindly Reply With Following Details:: TH THIlyas SafiNoch keine Bewertungen
- DLL On UNDERSTANDING DATA AND WAYS TO SYSTEMATICALLY COLLECT DATA - Research IIDokument3 SeitenDLL On UNDERSTANDING DATA AND WAYS TO SYSTEMATICALLY COLLECT DATA - Research IIRuffa L100% (1)
- DD309 Tma 05Dokument10 SeitenDD309 Tma 05papanombaNoch keine Bewertungen
- Oil Gas Midstream BFC 2018Dokument22 SeitenOil Gas Midstream BFC 2018zakaria aouamNoch keine Bewertungen
- Online FoodDokument8 SeitenOnline Foodneha agrawalNoch keine Bewertungen
- Sample CCSSADokument3 SeitenSample CCSSAiman_kundu2007756Noch keine Bewertungen
- ACYASR1 Syllabus T1-AY2023-2024Dokument13 SeitenACYASR1 Syllabus T1-AY2023-2024Janea Lorraine TanNoch keine Bewertungen