Das könnte Ihnen auch gefallen
- 2017 09 Ship Guidelines Vision ScreeningDokument38 Seiten2017 09 Ship Guidelines Vision ScreeningIsna SunintoNoch keine Bewertungen
- Australia-Avoidable Blindness and Vision LossDokument16 SeitenAustralia-Avoidable Blindness and Vision LossSi PuputNoch keine Bewertungen
- Prevalence of Diabetic Retinopathy and Blindness in Indonesian Adults With Type 2 DiabetesDokument29 SeitenPrevalence of Diabetic Retinopathy and Blindness in Indonesian Adults With Type 2 DiabetesSi PuputNoch keine Bewertungen
- AUSTRALIA SCREENING Cataract - Ccs - v17 - 1608for - Web - With - Va - Logo - by - CsDokument48 SeitenAUSTRALIA SCREENING Cataract - Ccs - v17 - 1608for - Web - With - Va - Logo - by - CsSi PuputNoch keine Bewertungen
- AMERICA-Regional Action Plan PAHODokument18 SeitenAMERICA-Regional Action Plan PAHOSi PuputNoch keine Bewertungen
- Blindness and Visual Impairment Situation in Indonesia Based On Rapid Assessment of Avoidable Blindness Surveys in 15 ProvincesDokument13 SeitenBlindness and Visual Impairment Situation in Indonesia Based On Rapid Assessment of Avoidable Blindness Surveys in 15 ProvincesSi Puput100% (1)
- INFOCUS MANUAL CATARACT SCREENINGF Primary-Eye-Care-Manual-Summary1Dokument21 SeitenINFOCUS MANUAL CATARACT SCREENINGF Primary-Eye-Care-Manual-Summary1Si PuputNoch keine Bewertungen
- Risk factors of diabetic retinopathy and vision threatening diabetic retinopathy and vision threatening diabetic retinopaty based on diabetic retinopathy screening program in greater bandung, west java.astriDokument14 SeitenRisk factors of diabetic retinopathy and vision threatening diabetic retinopathy and vision threatening diabetic retinopaty based on diabetic retinopathy screening program in greater bandung, west java.astriSi PuputNoch keine Bewertungen
- Towards Universal Eye Health Western PacificDokument28 SeitenTowards Universal Eye Health Western PacificSi PuputNoch keine Bewertungen
- AMERICA-Regional Action Plan PAHODokument18 SeitenAMERICA-Regional Action Plan PAHOSi PuputNoch keine Bewertungen
- Current Management of Vitreous Hemorrhage Due To Proliferative Diabetic RetinopathyDokument11 SeitenCurrent Management of Vitreous Hemorrhage Due To Proliferative Diabetic RetinopathySi PuputNoch keine Bewertungen
- Australia-Avoidable Blindness and Vision LossDokument16 SeitenAustralia-Avoidable Blindness and Vision LossSi PuputNoch keine Bewertungen
- Eye Health in The Commonwealth - Progress Report 2018 To 2020Dokument30 SeitenEye Health in The Commonwealth - Progress Report 2018 To 2020Si PuputNoch keine Bewertungen
- Changes in Ocular Growth After Pediatric Cataract SurgeryDokument11 SeitenChanges in Ocular Growth After Pediatric Cataract SurgerySi PuputNoch keine Bewertungen
- Epidemic Keratoconjunctivitis The Current SituatioDokument7 SeitenEpidemic Keratoconjunctivitis The Current SituatioSi PuputNoch keine Bewertungen
- Normal Postnatal Ocular DevelopmentDokument23 SeitenNormal Postnatal Ocular DevelopmentSi PuputNoch keine Bewertungen
- The Critical Period For Surgical Treatment of Dense Congenital Bilateral CataractsDokument5 SeitenThe Critical Period For Surgical Treatment of Dense Congenital Bilateral CataractsSi PuputNoch keine Bewertungen
- Pi Is 0140673616319791Dokument1 SeitePi Is 0140673616319791rendyjiwonoNoch keine Bewertungen
- Soal AceptDokument48 SeitenSoal AceptNova WidjanarkoNoch keine Bewertungen
- The Timing of Surgery For Congenital CataractsDokument6 SeitenThe Timing of Surgery For Congenital CataractsSi PuputNoch keine Bewertungen
- Duty Report 18 Januari 2020Dokument13 SeitenDuty Report 18 Januari 2020Si PuputNoch keine Bewertungen
- Reti No MetriDokument4 SeitenReti No MetriEstmar ValentinoNoch keine Bewertungen
- Systemic TherapyDokument8 SeitenSystemic TherapySi PuputNoch keine Bewertungen
- 2018 AAO Application-EnglishDokument2 Seiten2018 AAO Application-EnglishSi PuputNoch keine Bewertungen
- A Website - JOB Case ManagerDokument1 SeiteA Website - JOB Case ManagerWhina IndrianaNoch keine Bewertungen
- Prof. Clifford Hughes ISQuaDokument31 SeitenProf. Clifford Hughes ISQuaTri WidiastutiNoch keine Bewertungen
- 2018 AAO Application-EnglishDokument2 Seiten2018 AAO Application-EnglishSi PuputNoch keine Bewertungen
- New Doc 2018-05-04Dokument2 SeitenNew Doc 2018-05-04Si PuputNoch keine Bewertungen
- Care Plan Anak PDFDokument3 SeitenCare Plan Anak PDFSi PuputNoch keine Bewertungen
- Opth 10 179 PDFDokument8 SeitenOpth 10 179 PDFSi PuputNoch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- IATA Covid-19 - GuidanceDokument2 SeitenIATA Covid-19 - GuidanceMahashweta ChakrabortyNoch keine Bewertungen
- How Does Hypnosis Work Ebook Uncommon KnowledgeDokument12 SeitenHow Does Hypnosis Work Ebook Uncommon KnowledgeHarsh TripathiNoch keine Bewertungen
- Lectura Unidad 8Dokument16 SeitenLectura Unidad 8Day FuNoch keine Bewertungen
- Orthostatic Hypotension (Postural Hypotension) - Symptoms and Causes - Mayo ClinicDokument1 SeiteOrthostatic Hypotension (Postural Hypotension) - Symptoms and Causes - Mayo Clinicruba al hammadiNoch keine Bewertungen
- NeqasDokument2 SeitenNeqasMa. Theresa Enrile100% (1)
- CIMS Health Checkup Brochure (English) PDFDokument4 SeitenCIMS Health Checkup Brochure (English) PDFVaibhavNoch keine Bewertungen
- ATI Week 15Dokument4 SeitenATI Week 15Tee WoodNoch keine Bewertungen
- Life Spring, Case Study. 09.10.2010, For WEBDokument4 SeitenLife Spring, Case Study. 09.10.2010, For WEBanantisp2c2eNoch keine Bewertungen
- Scientific and Ethical Issues in The Use of Placebo Controls in Clinical TrialsDokument20 SeitenScientific and Ethical Issues in The Use of Placebo Controls in Clinical TrialsNicusor OnaciuNoch keine Bewertungen
- Application of Functional Orthodontic Appliances To Treatment of Mandibular Retrusion Syndrome PDFDokument18 SeitenApplication of Functional Orthodontic Appliances To Treatment of Mandibular Retrusion Syndrome PDFThu Trang Pham100% (1)
- A Clinical Report On Partial Pulpotomy and Capping With Calcium Hydroxide in Permanent Incisors With Complicated Crown FractureDokument6 SeitenA Clinical Report On Partial Pulpotomy and Capping With Calcium Hydroxide in Permanent Incisors With Complicated Crown Fractureroy sepNoch keine Bewertungen
- A Carbohydrate-Restrictive Strategy Is Safer and As Efficient As Intensive Insulin Therapy in Critically Ill PatientsDokument6 SeitenA Carbohydrate-Restrictive Strategy Is Safer and As Efficient As Intensive Insulin Therapy in Critically Ill PatientsTeresaNoch keine Bewertungen
- Antiespasmódicos - SimeticonaDokument8 SeitenAntiespasmódicos - SimeticonaCamilla CristinaNoch keine Bewertungen
- Session 4.1 Basic Concepts of Epidemiology: By: AS Ibrahim and NNH Mikhail, Ankara Cancer Epidemiology Course, April 2006Dokument30 SeitenSession 4.1 Basic Concepts of Epidemiology: By: AS Ibrahim and NNH Mikhail, Ankara Cancer Epidemiology Course, April 2006Benjamin PappuNoch keine Bewertungen
- Wellness Massage AssessmentDokument3 SeitenWellness Massage AssessmentElizabeth QuiderNoch keine Bewertungen
- Model State Medical Marijuana Bill PDFDokument26 SeitenModel State Medical Marijuana Bill PDFJoseph PreisterNoch keine Bewertungen
- Tmbool's Notes in Obstetrics and GynecologyDokument113 SeitenTmbool's Notes in Obstetrics and GynecologyFrom HumanNoch keine Bewertungen
- Anemia, Acute Bronchitis and Adequate NutritionDokument39 SeitenAnemia, Acute Bronchitis and Adequate NutritionSetiawan DanuNoch keine Bewertungen
- Hyperthermia HIV NURSING CARE PLAN FLODokument4 SeitenHyperthermia HIV NURSING CARE PLAN FLOMicaela CrisostomoNoch keine Bewertungen
- 2020 ISMP - Smart Infusion Pumps-FINALDokument38 Seiten2020 ISMP - Smart Infusion Pumps-FINALmochkurniawanNoch keine Bewertungen
- Mmha EcoDokument54 SeitenMmha EcoAlfredo De Ocampo JrNoch keine Bewertungen
- How To Calculate Calories Intake: by Group 6Dokument9 SeitenHow To Calculate Calories Intake: by Group 6Reina Magfirah MokogintaNoch keine Bewertungen
- Dci Journal PointsDokument1 SeiteDci Journal PointsRajesh Rathod0% (1)
- Prevalence and Recurrence Rate of Perianal Abscess - A Population-Based Study, Sweden 1997 - 2009Dokument5 SeitenPrevalence and Recurrence Rate of Perianal Abscess - A Population-Based Study, Sweden 1997 - 2009Ridha Aswina DalimuntheNoch keine Bewertungen
- SIP 2016 Abstract & Background Booklet V.6 PDFDokument187 SeitenSIP 2016 Abstract & Background Booklet V.6 PDFJimboreanu György PaulaNoch keine Bewertungen
- Treatment of Idiopathic Nephrotic Syndrome in Children - UpToDateDokument31 SeitenTreatment of Idiopathic Nephrotic Syndrome in Children - UpToDateChetra ColaNoch keine Bewertungen
- History of LaparosDokument27 SeitenHistory of LaparosDr. Sanjay KolteNoch keine Bewertungen
- ABCDE Assessment Exam: Eunice QuijanoDokument3 SeitenABCDE Assessment Exam: Eunice QuijanoQuijano GpokskieNoch keine Bewertungen
- Case Study 2Dokument19 SeitenCase Study 2Sumit Singh100% (1)
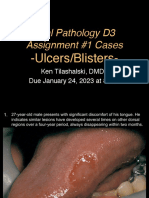
- D3 Ulcers Blisters Cases Due01242023 8amDokument13 SeitenD3 Ulcers Blisters Cases Due01242023 8amLinh PhanNoch keine Bewertungen