Das könnte Ihnen auch gefallen
- Thought Field TherapyDokument5 SeitenThought Field TherapyMitz VinegasNoch keine Bewertungen
- WI-962353 QEL03 Audit Plan LetterDokument3 SeitenWI-962353 QEL03 Audit Plan LetterChakky DestinyNoch keine Bewertungen
- The HDL Handbook: Biological Functions and Clinical ImplicationsVon EverandThe HDL Handbook: Biological Functions and Clinical ImplicationsNoch keine Bewertungen
- Confined Space: Hole Watch TrainingDokument36 SeitenConfined Space: Hole Watch TrainingMalik JunaidNoch keine Bewertungen
- Leachables Best Practice Guideline Disposable Solutions For Biomanufacturing PDFDokument36 SeitenLeachables Best Practice Guideline Disposable Solutions For Biomanufacturing PDFAziz Aditya Wiguna100% (2)
- Sagittal First - Ortho TribuneDokument8 SeitenSagittal First - Ortho TribuneOrtho OrganizersNoch keine Bewertungen
- MASUK MIAH POLAND AppointmentDokument3 SeitenMASUK MIAH POLAND Appointmentkaisarmukadam100% (1)
- Toxicity and Toxicokinetics of Metformin in RatsDokument26 SeitenToxicity and Toxicokinetics of Metformin in RatsPooja ReddyNoch keine Bewertungen
- Anima: Beyond Fantasy Character SheetDokument4 SeitenAnima: Beyond Fantasy Character SheetTristan TaksonNoch keine Bewertungen
- Femael Infertility PDFDokument9 SeitenFemael Infertility PDFAyadPalaniNoch keine Bewertungen
- Analytical Methods OriDokument18 SeitenAnalytical Methods OriHarsh KoshtiNoch keine Bewertungen
- Ajc 26 10 32Dokument3 SeitenAjc 26 10 32Deyinta Apenabel SuryaNoch keine Bewertungen
- Effects of Topical Application of Lipopolysaccharide and Proteases On Hepatic Injury Induced by High-Cholesterol Diet in RatsDokument7 SeitenEffects of Topical Application of Lipopolysaccharide and Proteases On Hepatic Injury Induced by High-Cholesterol Diet in RatsastrotactinNoch keine Bewertungen
- Plasma Homocysteine and Total Thiol Content in Patients With Exudative Age-Related Macular DegenerationDokument5 SeitenPlasma Homocysteine and Total Thiol Content in Patients With Exudative Age-Related Macular DegenerationAnonymous 1jCVqQuNoch keine Bewertungen
- Crystalloid For The Management of Burn Shock.: A Right Choice?Dokument15 SeitenCrystalloid For The Management of Burn Shock.: A Right Choice?syedsahibNoch keine Bewertungen
- 1 s2.0 S1570023208009343 Main PDFDokument5 Seiten1 s2.0 S1570023208009343 Main PDFmghaffarzadehNoch keine Bewertungen
- Glycolysis-Deficient: Studies Cells That Production of TumorDokument5 SeitenGlycolysis-Deficient: Studies Cells That Production of TumorFabian BalderrabanoNoch keine Bewertungen
- Jurnal 1Dokument5 SeitenJurnal 1Fafa RaraNoch keine Bewertungen
- CoenzymeQ10 Concentrations Breast Cancer PatientsDokument6 SeitenCoenzymeQ10 Concentrations Breast Cancer PatientsNikesh DoshiNoch keine Bewertungen
- Organochlorine Pesticide Residue Levels and Oxidative Stress in Preterm Delivery CasesDokument8 SeitenOrganochlorine Pesticide Residue Levels and Oxidative Stress in Preterm Delivery CasesSmita JainNoch keine Bewertungen
- GliclazideDokument8 SeitenGliclazideUpe VeerlapatiNoch keine Bewertungen
- Description of Reference Ranges for Organic Acids in Urine مهمDokument11 SeitenDescription of Reference Ranges for Organic Acids in Urine مهمfarkad rawiNoch keine Bewertungen
- SU22 4 2012 VelescuDokument6 SeitenSU22 4 2012 VelescuValentina AnutaNoch keine Bewertungen
- Journal of Chromatography B:, Rikard Landberg, Per Åman, Afaf Kamal-EldinDokument5 SeitenJournal of Chromatography B:, Rikard Landberg, Per Åman, Afaf Kamal-EldinNaeem YounisNoch keine Bewertungen
- 1 s2.0 S075333222100754X MainDokument4 Seiten1 s2.0 S075333222100754X MainMerrynda PutriNoch keine Bewertungen
- Intensive Care 1Dokument6 SeitenIntensive Care 1raitchuNoch keine Bewertungen
- Gjerde 2005Dokument9 SeitenGjerde 2005Desi TrirahmaNoch keine Bewertungen
- Petroianu 2005Dokument5 SeitenPetroianu 2005Bilel ChefiratNoch keine Bewertungen
- Iaft10i2p188 PDFDokument5 SeitenIaft10i2p188 PDFVirgo Eri SendiNoch keine Bewertungen
- Athyrium Multidentatum: Antioxidant Activity of Polysaccharides Extracted From (Doll) ChingDokument6 SeitenAthyrium Multidentatum: Antioxidant Activity of Polysaccharides Extracted From (Doll) ChingmeriemNoch keine Bewertungen
- Clinical Study: Serum Antioxidative Enzymes Levels and Oxidative Stress Products in Age-Related Cataract PatientsDokument7 SeitenClinical Study: Serum Antioxidative Enzymes Levels and Oxidative Stress Products in Age-Related Cataract PatientsStrangersNoch keine Bewertungen
- Pathogenesis of Preeclampsia: Implications of Apoptotic Markers and Oxidative StressDokument10 SeitenPathogenesis of Preeclampsia: Implications of Apoptotic Markers and Oxidative StressAchmad Deza FaristaNoch keine Bewertungen
- Extraction of Erythrocyte Enzymes For The Preparation of Polyhemoglobin-Catalase-Superoxide DismutaseDokument10 SeitenExtraction of Erythrocyte Enzymes For The Preparation of Polyhemoglobin-Catalase-Superoxide DismutaseIstván PortörőNoch keine Bewertungen
- Jurnal LisinoprilDokument7 SeitenJurnal LisinoprildidiisafitriNoch keine Bewertungen
- Effect of Organic Solvents Antigen Antibody InteractionsDokument7 SeitenEffect of Organic Solvents Antigen Antibody InteractionsMohammad RehanNoch keine Bewertungen
- Cloud-Point Extraction For The Determination of The Free Fraction of Antiepileptic Drugs in Blood Plasma and SalivaDokument5 SeitenCloud-Point Extraction For The Determination of The Free Fraction of Antiepileptic Drugs in Blood Plasma and SalivaDan AndonieNoch keine Bewertungen
- Related LiteratureDokument6 SeitenRelated LiteratureJean FlorencondiaNoch keine Bewertungen
- HPLC Method For Pharmacokinetics of Cis and Trans Isomer of Cefprozil Diastereomers in Human PlasmaDokument8 SeitenHPLC Method For Pharmacokinetics of Cis and Trans Isomer of Cefprozil Diastereomers in Human PlasmaIOSR Journal of PharmacyNoch keine Bewertungen
- IJFSTDokument7 SeitenIJFSTElavarasan KrishnamoorthyNoch keine Bewertungen
- Electron Spin Resonance SpectrosDokument6 SeitenElectron Spin Resonance SpectrossakuraleeshaoranNoch keine Bewertungen
- Eorop.a0Joor0a, Of: K. T. Kivistii and P. J. NeuvonenDokument4 SeitenEorop.a0Joor0a, Of: K. T. Kivistii and P. J. NeuvonenRoxanaLizettVillcaCastroNoch keine Bewertungen
- Oxidative Stress and Antioxidant Status in Acute Organophosphorous Insecticide PoisoningDokument5 SeitenOxidative Stress and Antioxidant Status in Acute Organophosphorous Insecticide PoisoningsakuraleeshaoranNoch keine Bewertungen
- 2012-Biomedical Chromatography-AppelDokument7 Seiten2012-Biomedical Chromatography-AppelHaojie ZhuNoch keine Bewertungen
- 17395137artif CellsDokument18 Seiten17395137artif CellsIstván PortörőNoch keine Bewertungen
- Plasma Malondialdehyde Level and Erythrocytes Catalase Activity in Patients With Type 2 Diabetes MellitusDokument14 SeitenPlasma Malondialdehyde Level and Erythrocytes Catalase Activity in Patients With Type 2 Diabetes MellitusKyae Mhon HtweNoch keine Bewertungen
- 1 s2.0 S002203021100213X MainDokument9 Seiten1 s2.0 S002203021100213X MainJuniClaudia13Noch keine Bewertungen
- Journal Lesitin RasioDokument3 SeitenJournal Lesitin RasioSUSANNoch keine Bewertungen
- Chen 2004Dokument8 SeitenChen 2004gtenienteNoch keine Bewertungen
- Pharmacokinetic Interaction Between Fluoxetine and Omeprazole in Healthy Male Volunteers: A Prospective Pilot StudyDokument9 SeitenPharmacokinetic Interaction Between Fluoxetine and Omeprazole in Healthy Male Volunteers: A Prospective Pilot StudyCurcubeuAuroraNoch keine Bewertungen
- Iyamu Et Al 2011Dokument8 SeitenIyamu Et Al 2011drojiehgodwinNoch keine Bewertungen
- Baillet, 2010 The Role of Oxidative StressDokument8 SeitenBaillet, 2010 The Role of Oxidative StressArlene AldreteNoch keine Bewertungen
- Glutathione Peroxidase Activity Assay With Colorimetric Method and Microplate Reading Format and Comparison With Chemiluminescence MethodDokument7 SeitenGlutathione Peroxidase Activity Assay With Colorimetric Method and Microplate Reading Format and Comparison With Chemiluminescence MethodAudrey LyliNoch keine Bewertungen
- Antihypertensive Effect of Quercetin in Rats Fed With A High Fat High Sucrose DietDokument8 SeitenAntihypertensive Effect of Quercetin in Rats Fed With A High Fat High Sucrose DietGabriel Oliveira de SouzaNoch keine Bewertungen
- Antioxidants 08 00142 PDFDokument11 SeitenAntioxidants 08 00142 PDFShahabuddinNoch keine Bewertungen
- Nutr 302 FinalprojectwithgradeDokument17 SeitenNutr 302 Finalprojectwithgradeapi-314354953Noch keine Bewertungen
- IJPPR, Vol8, Issue8 2016 (Jurnal Prakt 6)Dokument5 SeitenIJPPR, Vol8, Issue8 2016 (Jurnal Prakt 6)MUHAMAD ILFAN ALWIRUDIN IPBNoch keine Bewertungen
- Pathophysiology of Hypertrophic PyloricDokument9 SeitenPathophysiology of Hypertrophic PyloricVașadi Razvan CristianNoch keine Bewertungen
- Fechner 2001Dokument7 SeitenFechner 2001Daniel PmNoch keine Bewertungen
- Evaluation of Effect of Some Corticosteroids On Glucose-6-Phosphate Dehydrogenase and Comparative Study of Antioxidant Enzyme ActivitiesDokument6 SeitenEvaluation of Effect of Some Corticosteroids On Glucose-6-Phosphate Dehydrogenase and Comparative Study of Antioxidant Enzyme ActivitiesBrianna PowersNoch keine Bewertungen
- Amj-Hiponatremia Corregida Por Hiperglicemia-1999Dokument5 SeitenAmj-Hiponatremia Corregida Por Hiperglicemia-1999Mayra Alejandra Prada SerranoNoch keine Bewertungen
- LIPASEDokument4 SeitenLIPASEKresna Bondan FathoniNoch keine Bewertungen
- LeuprolideDokument7 SeitenLeuprolideMauricioNoch keine Bewertungen
- Relationship Serum and Saliva Chloramphenicol ConcentrationsDokument4 SeitenRelationship Serum and Saliva Chloramphenicol Concentrationsmonarch01Noch keine Bewertungen
- Effects of Thyroid Profile Changes On The Biochemical Markers of Bone, Liver and Renal Function in Non-Pregnant Women (Mohammad Yousaf PH.D)Dokument116 SeitenEffects of Thyroid Profile Changes On The Biochemical Markers of Bone, Liver and Renal Function in Non-Pregnant Women (Mohammad Yousaf PH.D)telecom valleyNoch keine Bewertungen
- Synthesis, Spectral Characterization and Bioactivity Studies of Some S-Substituted Derivatives of 5 - (4-Chlorophenyl) - 1,3,4-Oxadiazol-2-ThiolDokument9 SeitenSynthesis, Spectral Characterization and Bioactivity Studies of Some S-Substituted Derivatives of 5 - (4-Chlorophenyl) - 1,3,4-Oxadiazol-2-ThiolJing ZangNoch keine Bewertungen
- Intraplatelet Serotonin in Patients With Diabetes Mellitus and Peripheral Vascular DiseaseDokument6 SeitenIntraplatelet Serotonin in Patients With Diabetes Mellitus and Peripheral Vascular DiseaseHyeon DaNoch keine Bewertungen
- Trombositopenia Dan TrombositosisDokument33 SeitenTrombositopenia Dan TrombositosisAim AimmaNoch keine Bewertungen
- Anamnesis AnemiaDokument11 SeitenAnamnesis AnemiaAim AimmaNoch keine Bewertungen
- Anamnesis AnemiaDokument11 SeitenAnamnesis AnemiaAim AimmaNoch keine Bewertungen
- Lupus: Sigit Widyatmoko Fakultas Kedokteran UMSDokument52 SeitenLupus: Sigit Widyatmoko Fakultas Kedokteran UMSAim AimmaNoch keine Bewertungen
- Bismillahirobbil Alamien. Robbi Zidni Ilman: Sigit Widyatmoko Fakultas Kedokteran Universitas Muhammadiyah SurakartaDokument38 SeitenBismillahirobbil Alamien. Robbi Zidni Ilman: Sigit Widyatmoko Fakultas Kedokteran Universitas Muhammadiyah SurakartaAim AimmaNoch keine Bewertungen
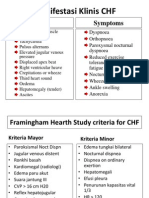
- Manifestasi Klinis CHF: Signs SymptomsDokument2 SeitenManifestasi Klinis CHF: Signs SymptomsAim AimmaNoch keine Bewertungen
- Construction and Validation of PS-FFQ (Parenting Style Four Factor Questionnaire)Dokument12 SeitenConstruction and Validation of PS-FFQ (Parenting Style Four Factor Questionnaire)Bernard CarpioNoch keine Bewertungen
- Disturbed Body Image FinalDokument2 SeitenDisturbed Body Image FinalHenry Philip0% (1)
- Ethics, Privacy, and SecurityDokument10 SeitenEthics, Privacy, and SecuritySittie Aina Munder100% (1)
- Ellen Respiratory Module PortraitDokument11 SeitenEllen Respiratory Module PortraitAbdelmar SusulanNoch keine Bewertungen
- Aaha Dental Guidelines PDFDokument21 SeitenAaha Dental Guidelines PDFGianfranco DanziNoch keine Bewertungen
- Luyando Nkwemu's Field ProjectDokument14 SeitenLuyando Nkwemu's Field ProjectMathews SikasoteNoch keine Bewertungen
- Rule 11: OR Exactly How Crazy Do I Need To Act To Get Out of Here?Dokument56 SeitenRule 11: OR Exactly How Crazy Do I Need To Act To Get Out of Here?Joshua Ling100% (2)
- Polysomnograph EnglishDokument5 SeitenPolysomnograph EnglishRam BehinNoch keine Bewertungen
- Pharmaceutical Jurisprudence Sovan Sarkar 186012111012Dokument11 SeitenPharmaceutical Jurisprudence Sovan Sarkar 186012111012Sovan SarkarNoch keine Bewertungen
- 1 SM PDFDokument4 Seiten1 SM PDFUtibe Tibz IkpembeNoch keine Bewertungen
- Helicobacter Pylori (PDFDrive)Dokument532 SeitenHelicobacter Pylori (PDFDrive)Susacande López GirónNoch keine Bewertungen
- Healthmedicinet Com II 2014 AugDokument400 SeitenHealthmedicinet Com II 2014 AugHeal ThmedicinetNoch keine Bewertungen
- Internship ProposalDokument3 SeitenInternship ProposalsrinivasNoch keine Bewertungen
- Experiment: Analysis of Milk: Output by Christian James MataDokument2 SeitenExperiment: Analysis of Milk: Output by Christian James MataSIJINoch keine Bewertungen
- (PDF) Pass Through Panic: Freeing Yourself From Anxiety and FearDokument1 Seite(PDF) Pass Through Panic: Freeing Yourself From Anxiety and FearmilonNoch keine Bewertungen
- Call Letter Specimen 2021 2022Dokument4 SeitenCall Letter Specimen 2021 2022Dr SahibaNoch keine Bewertungen
- Pencarrow Lighthouse Conservation PlanDokument98 SeitenPencarrow Lighthouse Conservation PlanClarice Futuro MuhlbauerNoch keine Bewertungen
- Inguinal Abscess Following CastrationDokument2 SeitenInguinal Abscess Following Castrationfahmi rosyadiNoch keine Bewertungen
- The 2030 Agenda For Sustainable Development and The "Five PS"Dokument2 SeitenThe 2030 Agenda For Sustainable Development and The "Five PS"Laraib ShahidNoch keine Bewertungen
- BCHEM Lab BreakdownDokument7 SeitenBCHEM Lab Breakdownsquishy23456Noch keine Bewertungen
- Diode Laser Therapy Systems: E-Beauty MachineDokument40 SeitenDiode Laser Therapy Systems: E-Beauty Machinekhaled khalasNoch keine Bewertungen
- Health Vocabulary ListDokument7 SeitenHealth Vocabulary ListClaudia MacarieNoch keine Bewertungen
- Medical Device Adverse Event Reporting Form: Materiovigilance Programme of India (Mvpi)Dokument4 SeitenMedical Device Adverse Event Reporting Form: Materiovigilance Programme of India (Mvpi)ashwani niteshNoch keine Bewertungen