Das könnte Ihnen auch gefallen
- Individual Case Study Acute GlomerulonephritisDokument26 SeitenIndividual Case Study Acute GlomerulonephritisBatrisyia HalimsNoch keine Bewertungen
- Case Study On Acute GlomerulonephritisDokument20 SeitenCase Study On Acute GlomerulonephritisJai - Ho87% (15)
- ESRD Secondary To Diabetic Nephropathy CASE STUDYDokument42 SeitenESRD Secondary To Diabetic Nephropathy CASE STUDYRalph Pelegrino75% (4)
- Acute PyelonephritisDokument59 SeitenAcute PyelonephritisKylie Golindang100% (1)
- Case AGNDokument66 SeitenCase AGNMohaima PanditaNoch keine Bewertungen
- Case Study: Acute GlomerulonephritisDokument19 SeitenCase Study: Acute GlomerulonephritisKuruma Maricar SorianoNoch keine Bewertungen
- Acute Renal FailureDokument59 SeitenAcute Renal Failurepaul_v_44440% (1)
- Case Study: Acute GlomerulonephritisDokument28 SeitenCase Study: Acute GlomerulonephritisMa Rafaela Rosales Palompon91% (11)
- Acute Glomerulonephritis Case StudyDokument12 SeitenAcute Glomerulonephritis Case StudyPrincess Tindugan100% (1)
- NCP AgnDokument2 SeitenNCP AgnMichael Vincent DuroNoch keine Bewertungen
- Case Study - Acute Glomerulonephritis Sample Case Study Report For PCL Level by Amrit BanstolaDokument15 SeitenCase Study - Acute Glomerulonephritis Sample Case Study Report For PCL Level by Amrit BanstolaAmrit Banstola100% (5)
- Case Study CKD DM Type 2Dokument7 SeitenCase Study CKD DM Type 2Brian Cornel0% (3)
- Chronic Kidney Disease Stage 5Dokument21 SeitenChronic Kidney Disease Stage 5Kristine Anne Soriano100% (1)
- Case Study On Chronic Kidney DiseaseDokument9 SeitenCase Study On Chronic Kidney DiseaseHalles Beverlyn Crisostomo GeraldeNoch keine Bewertungen
- Case StudyDokument37 SeitenCase StudyAnonymous t78m8ku100% (1)
- Acute Glomerulonephritis - CSDokument31 SeitenAcute Glomerulonephritis - CSMASIINoch keine Bewertungen
- Acute Glomerulonephritis GCDokument70 SeitenAcute Glomerulonephritis GCMary Cruz100% (2)
- University of Perpetual Help System DALTA: College of Radiologic TechnologyDokument3 SeitenUniversity of Perpetual Help System DALTA: College of Radiologic TechnologyJynrose Kaye GulpanyNoch keine Bewertungen
- Diabetic Ketoacidosis: Albano, Bautista, Cimatu, Purificacion, SieteralesDokument84 SeitenDiabetic Ketoacidosis: Albano, Bautista, Cimatu, Purificacion, SieteralesSyd BautistaNoch keine Bewertungen
- Hydronephrosis Fred LuceDokument69 SeitenHydronephrosis Fred LuceKMNoch keine Bewertungen
- Community Diagnosis NCM 113 2Dokument63 SeitenCommunity Diagnosis NCM 113 2Jewenson SalvadorNoch keine Bewertungen
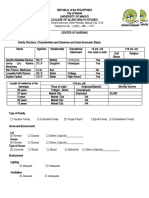
- Family Structure and Socio-Economic Status QuestionnaireDokument4 SeitenFamily Structure and Socio-Economic Status QuestionnaireLouwella RamosNoch keine Bewertungen
- Case StudyDokument26 SeitenCase Studyamazing grace mejia carlos100% (2)
- Case PresentationDokument10 SeitenCase PresentationWina Hanriyani0% (1)
- Case Study 1 FinalDokument28 SeitenCase Study 1 Finalapi-3905968320% (1)
- Acute GlumerulonephritisDokument77 SeitenAcute GlumerulonephritisNicoleNoch keine Bewertungen
- Case Study DMDokument48 SeitenCase Study DMBenj Villanueva100% (1)
- NCP AgnDokument2 SeitenNCP Agnj3nann3Noch keine Bewertungen
- Acute Glomerulonephritis 42-mDokument27 SeitenAcute Glomerulonephritis 42-mcbanguisNoch keine Bewertungen
- Nephrotic SyndromeDokument61 SeitenNephrotic SyndromeRanah Julia Garchitorena AyoNoch keine Bewertungen
- Nursing care plan for impaired nutrition and tissue integrityDokument11 SeitenNursing care plan for impaired nutrition and tissue integrityRaidis PangilinanNoch keine Bewertungen
- Case Study About Type II Diabetes MellitusDokument82 SeitenCase Study About Type II Diabetes MellitusKristine YoungNoch keine Bewertungen
- Chronic Kidney Disease Case StudyDokument52 SeitenChronic Kidney Disease Case StudyGi100% (1)
- Pathophysiology of Gestational DMDokument3 SeitenPathophysiology of Gestational DMAnonymous GtR96jCNoch keine Bewertungen
- Pathophysiology of Acute GastroenteritisDokument5 SeitenPathophysiology of Acute Gastroenteritisheron_bayanin_15Noch keine Bewertungen
- CHF Case Study on Congestive Heart FailureDokument40 SeitenCHF Case Study on Congestive Heart Failurelyndzy100% (1)
- NCP HyperthermiaDokument3 SeitenNCP HyperthermiaDhonabelleVanessaFetalinoAdona100% (1)
- NURSING Nursing Care Plan for Diabetes MellitusDokument3 SeitenNURSING Nursing Care Plan for Diabetes MellitusYsun Espino100% (1)
- Acute Glomerulonephritis Case StudyDokument12 SeitenAcute Glomerulonephritis Case Study19lyon92100% (6)
- Renal Calculi Case Study Spring 2007Dokument2 SeitenRenal Calculi Case Study Spring 2007niting110% (1)
- CKD (F&e)Dokument110 SeitenCKD (F&e)Al-nazer Azer Al100% (1)
- DM - Case Pres 1aDokument59 SeitenDM - Case Pres 1abon clayNoch keine Bewertungen
- Acute Gastroenteritis Case StudyDokument20 SeitenAcute Gastroenteritis Case StudyJohn Carlo Kimura Rabanes100% (1)
- Gastroenteritis: Causes, Symptoms, and Treatment of Stomach FluDokument49 SeitenGastroenteritis: Causes, Symptoms, and Treatment of Stomach Flukinasal21Noch keine Bewertungen
- Case Analysis FinalDokument29 SeitenCase Analysis FinalVeyNoch keine Bewertungen
- Case Study 18 CKDDokument7 SeitenCase Study 18 CKDapi-301049551Noch keine Bewertungen
- Pregnancy Induced Hypertension PathophysiologyDokument2 SeitenPregnancy Induced Hypertension PathophysiologyCamille Grace100% (1)
- Case Study of Cesarean SectionDokument9 SeitenCase Study of Cesarean SectionErika Joy Imperio0% (1)
- SOAPIEDokument34 SeitenSOAPIEEm Castillo100% (1)
- Mechanisms Case StudyDokument13 SeitenMechanisms Case Studyshane_tin143Noch keine Bewertungen
- Case Analysis: Republic of The Philippines Bicol UniversityDokument7 SeitenCase Analysis: Republic of The Philippines Bicol UniversityTrixia AlmendralNoch keine Bewertungen
- Chronic Kidney Disease Case PresDokument32 SeitenChronic Kidney Disease Case Presnnaesor_1091Noch keine Bewertungen
- Case Study 10 Renal FailureDokument19 SeitenCase Study 10 Renal FailureAriadne Cordelette100% (2)
- Deficient Fluid VolumeDokument1 SeiteDeficient Fluid VolumeSheila ErpeloNoch keine Bewertungen
- Case StudyDokument41 SeitenCase StudyAubrey Ann FolloscoNoch keine Bewertungen
- Grand Case Study FinalDokument34 SeitenGrand Case Study FinalFenina S. CalmaNoch keine Bewertungen
- Gastroenterology For General SurgeonsVon EverandGastroenterology For General SurgeonsMatthias W. WichmannNoch keine Bewertungen
- Colorectal CancerDokument50 SeitenColorectal CancerHans Chester Rirao Capinding100% (2)
- Certificate of Appearance: Melascom O. Malicay Van Vugt Project StafDokument1 SeiteCertificate of Appearance: Melascom O. Malicay Van Vugt Project StafMonique ReyesNoch keine Bewertungen
- English RevisionDokument5 SeitenEnglish RevisionMonique ReyesNoch keine Bewertungen
- Worship Workshop: ZahpoiDokument9 SeitenWorship Workshop: ZahpoiMonique ReyesNoch keine Bewertungen
- OBESITYDokument21 SeitenOBESITYMonique ReyesNoch keine Bewertungen
- English RevisionDokument5 SeitenEnglish RevisionMonique ReyesNoch keine Bewertungen
- Allergic Rhinitis in Children Power Point PresentationDokument45 SeitenAllergic Rhinitis in Children Power Point PresentationMonique ReyesNoch keine Bewertungen
- God Is EnoughDokument13 SeitenGod Is EnoughMonique ReyesNoch keine Bewertungen
- Organic ChemistryDokument17 SeitenOrganic ChemistryMonique ReyesNoch keine Bewertungen
- Discomforts of Middle To Late PregnancyDokument18 SeitenDiscomforts of Middle To Late PregnancyMonique ReyesNoch keine Bewertungen
- Two Greek Philosophers Plato & AristotleDokument15 SeitenTwo Greek Philosophers Plato & AristotleMonique ReyesNoch keine Bewertungen
- Critical Care ApplicationDokument36 SeitenCritical Care ApplicationMonique ReyesNoch keine Bewertungen
- COPD and Asthma: Causes, Symptoms, Diagnosis and TreatmentDokument138 SeitenCOPD and Asthma: Causes, Symptoms, Diagnosis and TreatmentMonique Reyes0% (1)
- Discomforts of Middle To Late PregnancyDokument18 SeitenDiscomforts of Middle To Late PregnancyMonique ReyesNoch keine Bewertungen
- NursingDokument15 SeitenNursingMonique ReyesNoch keine Bewertungen
- Case Study PsychDokument49 SeitenCase Study PsychMonique Reyes100% (1)
- Four Levels of Protein StructureDokument9 SeitenFour Levels of Protein StructureMonique ReyesNoch keine Bewertungen
- Acute Pain AGEDokument2 SeitenAcute Pain AGEHarris AustriaNoch keine Bewertungen
- Renal Anatomy & Physiology OverviewDokument5 SeitenRenal Anatomy & Physiology OverviewChristopher BucuNoch keine Bewertungen
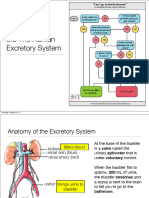
- SBI4U Unit 4 Homeostasis Excretory SystemDokument27 SeitenSBI4U Unit 4 Homeostasis Excretory System전채연Noch keine Bewertungen
- (PHYSIO B) 1.2 Renal Physio Pt. 3Dokument8 Seiten(PHYSIO B) 1.2 Renal Physio Pt. 3miguel cuevasNoch keine Bewertungen
- Anatomy, Abdomen and Pelvis, Kidneys: Statpearls (Internet) - Treasure Island (FL) : Statpearls Publishing 2022 JanDokument6 SeitenAnatomy, Abdomen and Pelvis, Kidneys: Statpearls (Internet) - Treasure Island (FL) : Statpearls Publishing 2022 Janvenus ohNoch keine Bewertungen
- CH 28Dokument22 SeitenCH 28Jann Zaniel Allayne RiNoch keine Bewertungen
- Renal: Est Autoregulatory SystemsDokument12 SeitenRenal: Est Autoregulatory SystemsIdrissa ContehNoch keine Bewertungen
- Physio - Water BalanceDokument8 SeitenPhysio - Water Balanceavian_rose100% (2)
- Excretory System (Quizziz)Dokument6 SeitenExcretory System (Quizziz)mariaNoch keine Bewertungen
- Ch18 Lecture PPT ADokument70 SeitenCh18 Lecture PPT AMiky rose De Guzman100% (1)
- Kidney Nephron Structure and FunctionDokument4 SeitenKidney Nephron Structure and Functionxanxan4321Noch keine Bewertungen
- Animal Physiology AssignmentDokument26 SeitenAnimal Physiology AssignmentAnjali MunjalNoch keine Bewertungen
- CKD Case AnalysisDokument25 SeitenCKD Case Analysisしゃいな ふかみNoch keine Bewertungen
- DiureticDokument40 SeitenDiuretichoneyworksNoch keine Bewertungen
- Introduction and Assessment of The Renal - Urological SystemDokument182 SeitenIntroduction and Assessment of The Renal - Urological SystemValerie Suge-Michieka100% (1)
- Bio-Zoology - Vol - 2 EM PDFDokument176 SeitenBio-Zoology - Vol - 2 EM PDFmuraliNoch keine Bewertungen
- Kidney Structure and FunctionDokument18 SeitenKidney Structure and Functionalisha khanNoch keine Bewertungen
- Acid-Base and Potassium HomeostasisDokument8 SeitenAcid-Base and Potassium HomeostasisVeronica WongNoch keine Bewertungen
- IAL Biology SB2 Answers 7CDokument7 SeitenIAL Biology SB2 Answers 7CsalmaNoch keine Bewertungen
- Kidney Function: What Do The Kidneys Do?Dokument4 SeitenKidney Function: What Do The Kidneys Do?A Mazid Zabir IINoch keine Bewertungen
- The Whole Enchilada PDFDokument602 SeitenThe Whole Enchilada PDFMr XNoch keine Bewertungen
- Lab Report Exp 2 - Kidney Function & Physiology (Group 4)Dokument10 SeitenLab Report Exp 2 - Kidney Function & Physiology (Group 4)FARHAH BATRISYIA ABDUL RAHIMNoch keine Bewertungen
- JAM 2022 Biotechnology QuestionsDokument28 SeitenJAM 2022 Biotechnology QuestionsKumar KalyanNoch keine Bewertungen
- Lecture Notes On The Renal System-1Dokument51 SeitenLecture Notes On The Renal System-1GiftedNoch keine Bewertungen
- Chapter No. 15 - Homeostasis (By Faisal Zada Khan)Dokument36 SeitenChapter No. 15 - Homeostasis (By Faisal Zada Khan)Pubg Killer15Noch keine Bewertungen
- Anatomy of the Heart - Layers, Chambers, ValvesDokument28 SeitenAnatomy of the Heart - Layers, Chambers, ValvesHerman DjawaNoch keine Bewertungen
- Study QuestionDokument24 SeitenStudy QuestionEbookslatinosEbookslatinosNoch keine Bewertungen
- Renal MCQ 2Dokument6 SeitenRenal MCQ 2AzizNoch keine Bewertungen
- Urine FormationDokument49 SeitenUrine FormationMajd HusseinNoch keine Bewertungen
- CM Review. Urinalysis and Renal Disorders 2Dokument19 SeitenCM Review. Urinalysis and Renal Disorders 2Sarah EugenioNoch keine Bewertungen
- Chapter 18 URINARY SYSTEM SeeleysDokument106 SeitenChapter 18 URINARY SYSTEM SeeleysAlvinTercianoVitugNoch keine Bewertungen