Das könnte Ihnen auch gefallen
- Medical Parasitology QuestionsDokument5 SeitenMedical Parasitology Questionsskeltenboi74% (19)
- Annotated Bibliography 2Dokument6 SeitenAnnotated Bibliography 2api-292066378Noch keine Bewertungen
- DengueDokument34 SeitenDengueNa YamzonNoch keine Bewertungen
- 040 27736am101214 311 314Dokument4 Seiten040 27736am101214 311 314Finka InaraeNoch keine Bewertungen
- 2012 Number 1 947445146213461Dokument5 Seiten2012 Number 1 947445146213461MedstudNoch keine Bewertungen
- Article1380102045 - Sebastian Et AlDokument4 SeitenArticle1380102045 - Sebastian Et AlAndrea RivaNoch keine Bewertungen
- Congenital CMV Infection in Symptomatic Infants in Delhi and Surrounding AreasDokument3 SeitenCongenital CMV Infection in Symptomatic Infants in Delhi and Surrounding AreasMinerva StanciuNoch keine Bewertungen
- Preliminary Report of Hiv and Toxoplasma Gondii Occurrence in Pregnant Women From MozambiqueDokument5 SeitenPreliminary Report of Hiv and Toxoplasma Gondii Occurrence in Pregnant Women From MozambiqueBla BlaNoch keine Bewertungen
- Impact of Malaria at The End of Pregnancy On Infant Mortality and MorbidityDokument9 SeitenImpact of Malaria at The End of Pregnancy On Infant Mortality and MorbidityDebby Astasya AnnisaNoch keine Bewertungen
- Dengue Infection During Pregnancy andDokument7 SeitenDengue Infection During Pregnancy andAlia SalviraNoch keine Bewertungen
- 83865-Article Text-203346-1-10-20121213 PDFDokument5 Seiten83865-Article Text-203346-1-10-20121213 PDFosama musaNoch keine Bewertungen
- Vertical Transmission of Dengue Virus in The Peripartum Period and Viral Kinetics in Newborns and Breast Milk: New DataDokument8 SeitenVertical Transmission of Dengue Virus in The Peripartum Period and Viral Kinetics in Newborns and Breast Milk: New DataMarcelo QuipildorNoch keine Bewertungen
- Epidemiology of TORCH Infections and Understanding The Serology in Their DiagnosisDokument5 SeitenEpidemiology of TORCH Infections and Understanding The Serology in Their DiagnosisEllya Syahfitri 2108125983Noch keine Bewertungen
- DiagnosisofpulmonaryTB in ChildrenDokument8 SeitenDiagnosisofpulmonaryTB in ChildrenSumit MitraNoch keine Bewertungen
- MorbiliDokument7 SeitenMorbilijourey08Noch keine Bewertungen
- Cong InfDokument72 SeitenCong InffarazNoch keine Bewertungen
- Further Efforts in The Achievement of Congenital Rubella Syndrome/rubella EliminationDokument5 SeitenFurther Efforts in The Achievement of Congenital Rubella Syndrome/rubella Eliminationfpm5948Noch keine Bewertungen
- Prevalence and Incidence of Dengue Virus and Antibody Placental Transfer During Late Pregnancy in Central BrazilDokument7 SeitenPrevalence and Incidence of Dengue Virus and Antibody Placental Transfer During Late Pregnancy in Central Brazilrgutierrez1722Noch keine Bewertungen
- Ijpa 18 93Dokument7 SeitenIjpa 18 93Frank Barreiro SanchezNoch keine Bewertungen
- Research Article Toxoplasma Gondii Amongst Pregnant: Seroepidemiology of Women in Jazan Province, Saudi ArabiaDokument7 SeitenResearch Article Toxoplasma Gondii Amongst Pregnant: Seroepidemiology of Women in Jazan Province, Saudi ArabiaMAHFOUZ2015Noch keine Bewertungen
- Hypoglycemia and Anemia Associated With Malaria Among Pregnant Mothers Living With HIV Attending Aminu Kano Teaching Hospital, Kano State-NigeriaDokument6 SeitenHypoglycemia and Anemia Associated With Malaria Among Pregnant Mothers Living With HIV Attending Aminu Kano Teaching Hospital, Kano State-NigeriaUMYU Journal of Microbiology Research (UJMR)Noch keine Bewertungen
- Medicine - IJGMP - HUMAN IMMUNO DEFFICIENCY - Adetunji Oladeni Adeniji - NigeriaDokument10 SeitenMedicine - IJGMP - HUMAN IMMUNO DEFFICIENCY - Adetunji Oladeni Adeniji - Nigeriaiaset123Noch keine Bewertungen
- Fneur 04 00142Dokument7 SeitenFneur 04 00142nyuwwchocolavaNoch keine Bewertungen
- Navti 2016Dokument7 SeitenNavti 2016XXXI-JKhusnan Mustofa GufronNoch keine Bewertungen
- Dengue in Pregnancy: An Under-Reported Illness, With Special Reference To Other Existing Co-InfectionsDokument3 SeitenDengue in Pregnancy: An Under-Reported Illness, With Special Reference To Other Existing Co-InfectionsLeonardoMartínezNoch keine Bewertungen
- Hubungan Infeksi Torch Pada Kehamilan Dengan Kejadian Kelainan Kongenital Pada Bayi Baru LahirDokument11 SeitenHubungan Infeksi Torch Pada Kehamilan Dengan Kejadian Kelainan Kongenital Pada Bayi Baru LahirSepthianingsiNoch keine Bewertungen
- Evidence 3) Congenital Infection Causes Neurologic and Hematologic Damage andDokument5 SeitenEvidence 3) Congenital Infection Causes Neurologic and Hematologic Damage andandamar0290Noch keine Bewertungen
- The Global Burden of Congenital ToxoplasmosisDokument10 SeitenThe Global Burden of Congenital ToxoplasmosisLuis Andrés Guaicha AlvaradoNoch keine Bewertungen
- Toxoplasma and RubellaDokument37 SeitenToxoplasma and RubellaHervi LaksariNoch keine Bewertungen
- Knowledge and Perception of Female Nursing Students About Human Papilloma Virus (HPV), Cervical Cancer and Attitudes Towards HPV VaccinationDokument18 SeitenKnowledge and Perception of Female Nursing Students About Human Papilloma Virus (HPV), Cervical Cancer and Attitudes Towards HPV VaccinationpangaribuansantaNoch keine Bewertungen
- Gonorrhoe Pregnancy ChildrenDokument5 SeitenGonorrhoe Pregnancy ChildrenWidya Derattano Pikal LimNoch keine Bewertungen
- Citomegalovirus - Primoinfección & Embarazo - Picone 2013Dokument8 SeitenCitomegalovirus - Primoinfección & Embarazo - Picone 2013Rolando LaraNoch keine Bewertungen
- Articles: BackgroundDokument9 SeitenArticles: BackgroundRendra Artha Ida BagusNoch keine Bewertungen
- TORCH Infection in Pregnant Women Ver September 2017 PDFDokument9 SeitenTORCH Infection in Pregnant Women Ver September 2017 PDFRevina AmaliaNoch keine Bewertungen
- Tuberculosis and PregnancyDokument22 SeitenTuberculosis and PregnancyHendra PranataNoch keine Bewertungen
- Screening Options in The Management of Congenital ToxoplasmosisDokument3 SeitenScreening Options in The Management of Congenital ToxoplasmosisannaNoch keine Bewertungen
- Toxoplasma y Citomehalovirus PDFDokument12 SeitenToxoplasma y Citomehalovirus PDFGUSTAVO ANDRES NORENA LOPEZNoch keine Bewertungen
- CMV VirusDokument8 SeitenCMV VirusKalpavriksha1974Noch keine Bewertungen
- 1 s2.0 S2214109X14703304 MainDokument7 Seiten1 s2.0 S2214109X14703304 MainAura NirwanaNoch keine Bewertungen
- MAKALAH Keputusasan-1Dokument7 SeitenMAKALAH Keputusasan-1ARINANoch keine Bewertungen
- Hubungan Infeksi Torch Pada Kehamilan Dengan Kejadian Kelainan Kongenital Pada Bayi Baru LahirDokument10 SeitenHubungan Infeksi Torch Pada Kehamilan Dengan Kejadian Kelainan Kongenital Pada Bayi Baru LahirIkramuna AFNoch keine Bewertungen
- Maternal SepsisDokument9 SeitenMaternal Sepsispamela tyas milanaNoch keine Bewertungen
- Osman 2017Dokument32 SeitenOsman 2017Adrian Quiroga RodriguezNoch keine Bewertungen
- Changes in The Utilization of Prenatal Diagnosis.19Dokument6 SeitenChanges in The Utilization of Prenatal Diagnosis.19Filipa DiasNoch keine Bewertungen
- 282 F 4 e 2 Edaf 124 A 0Dokument12 Seiten282 F 4 e 2 Edaf 124 A 0Mazin AlmaziniNoch keine Bewertungen
- Ijpedi2021 1544553Dokument6 SeitenIjpedi2021 1544553Naresh ReddyNoch keine Bewertungen
- Original Research ArticlesDokument7 SeitenOriginal Research Articlessalma romnalia ashshofaNoch keine Bewertungen
- Karakteristik Penderita Sepsis Neonatorum Rawat Inap Di Rsud Dr. Pirngadi Medan TAHUN 2010-2011Dokument10 SeitenKarakteristik Penderita Sepsis Neonatorum Rawat Inap Di Rsud Dr. Pirngadi Medan TAHUN 2010-2011meriatmajaNoch keine Bewertungen
- 235 Article 637 1 10 20180924Dokument8 Seiten235 Article 637 1 10 20180924Mazin AlmaziniNoch keine Bewertungen
- Congenital Cytomegalovirus Infection Clinical Features and DiagnosisDokument21 SeitenCongenital Cytomegalovirus Infection Clinical Features and Diagnosisgomitas21Noch keine Bewertungen
- Jurnal LeukoreaDokument6 SeitenJurnal LeukoreaLystiani Puspita DewiNoch keine Bewertungen
- Dengue Infections During Pregnancy: Case Series From A Tertiary Care Hospital in Sri LankaDokument9 SeitenDengue Infections During Pregnancy: Case Series From A Tertiary Care Hospital in Sri LankaYan Sheng HoNoch keine Bewertungen
- Epidemiology and Clinical Characteristic of Patient Acute Gastroenteritis (AGEDokument12 SeitenEpidemiology and Clinical Characteristic of Patient Acute Gastroenteritis (AGEGusdek AryaNoch keine Bewertungen
- 7.Applied-ELISA and ICT Techniques in The Detection of Anti - Rubella - Intidhaar N. Abid 123Dokument6 Seiten7.Applied-ELISA and ICT Techniques in The Detection of Anti - Rubella - Intidhaar N. Abid 123Impact JournalsNoch keine Bewertungen
- Management of Varicella Infection (Chickenpox) in Pregnancy: Sogc Clinical Practice GuidelineDokument6 SeitenManagement of Varicella Infection (Chickenpox) in Pregnancy: Sogc Clinical Practice GuidelineAndi NugrohoNoch keine Bewertungen
- Recommended Management of Toxoplasma Gondii Infection in Pregnant Women and Their ChildrenDokument12 SeitenRecommended Management of Toxoplasma Gondii Infection in Pregnant Women and Their Childrenakanksha nagarNoch keine Bewertungen
- First Colombian Multicentric Newborn Screening For Congenital ToxoplasmosisDokument10 SeitenFirst Colombian Multicentric Newborn Screening For Congenital ToxoplasmosisFrontiersNoch keine Bewertungen
- Maedica 15 253Dokument5 SeitenMaedica 15 253Fer AguilarNoch keine Bewertungen
- Zidovudina IntrapartumDokument12 SeitenZidovudina Intrapartumsara lopezNoch keine Bewertungen
- Case Report: Severe Congenital Toxoplasmosis: A Case Report and Strain CharacterizationDokument4 SeitenCase Report: Severe Congenital Toxoplasmosis: A Case Report and Strain CharacterizationNamanamanaNoch keine Bewertungen
- Paediatrica Indonesiana: Darnifayanti, Guslihan Dasa Tjipta, Rusdidjas, Bugis Mardina LubisDokument5 SeitenPaediatrica Indonesiana: Darnifayanti, Guslihan Dasa Tjipta, Rusdidjas, Bugis Mardina LubisQonitina HafidhaNoch keine Bewertungen
- Guide to Pediatric Urology and Surgery in Clinical PracticeVon EverandGuide to Pediatric Urology and Surgery in Clinical PracticeNoch keine Bewertungen
- Management of Tuberculosis: A guide for clinicians (eBook edition)Von EverandManagement of Tuberculosis: A guide for clinicians (eBook edition)Noch keine Bewertungen
- WvdcwsvsDokument1 SeiteWvdcwsvsKrishna WijayaNoch keine Bewertungen
- OuunjjDokument7 SeitenOuunjjKrishna WijayaNoch keine Bewertungen
- Traktus2 Sing Ptg2 IkiDokument25 SeitenTraktus2 Sing Ptg2 IkiKrishna WijayaNoch keine Bewertungen
- Artikulasio SeeleyDokument18 SeitenArtikulasio SeeleyKrishna WijayaNoch keine Bewertungen
- An Epidemiological Study of Traumatic Brachial Plexus Injury Patients Treated at An Indian CentreDokument8 SeitenAn Epidemiological Study of Traumatic Brachial Plexus Injury Patients Treated at An Indian CentreKrishna WijayaNoch keine Bewertungen
- Manual For The Surveillance of Vaccigsne-Preventable Diseases - Mumps (CDC)Dokument14 SeitenManual For The Surveillance of Vaccigsne-Preventable Diseases - Mumps (CDC)Krishna WijayaNoch keine Bewertungen
- Manual For The Surveillance of Vaccigsne-Preventable Diseases - Mumps (CDC)Dokument14 SeitenManual For The Surveillance of Vaccigsne-Preventable Diseases - Mumps (CDC)Krishna WijayaNoch keine Bewertungen
- Asd 1Dokument4 SeitenAsd 1Krishna WijayaNoch keine Bewertungen
- Automated Degenerate PCR Primer Design For High-Throughput Sequencing Improves Efficiency of Viral SequencingDokument9 SeitenAutomated Degenerate PCR Primer Design For High-Throughput Sequencing Improves Efficiency of Viral SequencingKrishna WijayaNoch keine Bewertungen
- WHO Dengue Guidelines 2013Dokument160 SeitenWHO Dengue Guidelines 2013Jason MirasolNoch keine Bewertungen
- Practical Guidelines Infection Control PDFDokument110 SeitenPractical Guidelines Infection Control PDFRao Rizwan Shakoor100% (1)
- Microbial Diseases of The Digestive SystemDokument150 SeitenMicrobial Diseases of The Digestive Systemone_nd_onlyuNoch keine Bewertungen
- Dengue Syndrome: Presented By: A.Sahaya Mary M.SC Nursing I Yr Scon, SimatsDokument57 SeitenDengue Syndrome: Presented By: A.Sahaya Mary M.SC Nursing I Yr Scon, Simatssagi muNoch keine Bewertungen
- Protozoa (Q) PDFDokument4 SeitenProtozoa (Q) PDFBhupesh ChandNoch keine Bewertungen
- Table For BacteriaDokument2 SeitenTable For BacteriaSnow best budNoch keine Bewertungen
- Covid PresentationDokument21 SeitenCovid Presentationchici azriniNoch keine Bewertungen
- Upper Respiratory Tract Infection (Uri)Dokument4 SeitenUpper Respiratory Tract Infection (Uri)Anna Zhifa AbNoch keine Bewertungen
- Laporan Vaksin 01112021 OkeDokument1.077 SeitenLaporan Vaksin 01112021 OkeThewie ApydNoch keine Bewertungen
- Cloze Test PracticeDokument3 SeitenCloze Test PracticeNico ScoNoch keine Bewertungen
- Position PaperDokument8 SeitenPosition Paperapi-316749075Noch keine Bewertungen
- Preventing Needlestick Injuries Among Healthcare Workers:: A WHO-ICN CollaborationDokument6 SeitenPreventing Needlestick Injuries Among Healthcare Workers:: A WHO-ICN CollaborationWasni TheresiaNoch keine Bewertungen
- Inocencio School Student Health Declaration SheetDokument2 SeitenInocencio School Student Health Declaration SheetCrunchy Fried RiceNoch keine Bewertungen
- Daftar Pustaka Prevertebral THTDokument3 SeitenDaftar Pustaka Prevertebral THTqys90Noch keine Bewertungen
- (PPT) DPC 1.4.2 Immunity and Disease - Dr. Cabanos PDFDokument83 Seiten(PPT) DPC 1.4.2 Immunity and Disease - Dr. Cabanos PDFJennifer Pisco LiracNoch keine Bewertungen
- Isolation Guidelines PDFDokument209 SeitenIsolation Guidelines PDFlimiya vargheseNoch keine Bewertungen
- Intructions:: 1. Make A Summary of Key Reactions For EnterobacteriaceaeDokument3 SeitenIntructions:: 1. Make A Summary of Key Reactions For EnterobacteriaceaeMare5Der5Noch keine Bewertungen
- The All-Frequencies CAFL (AFCAFL)Dokument27 SeitenThe All-Frequencies CAFL (AFCAFL)Federico Ceriani100% (1)
- Tuberculosis Thesis TopicsDokument7 SeitenTuberculosis Thesis Topicsstacyjohnsonreno100% (2)
- Cefepime Vs Zosyn For Empiric Sepsis CoverageDokument2 SeitenCefepime Vs Zosyn For Empiric Sepsis Coveragetl drNoch keine Bewertungen
- A Secondary Yeast Infection: Student WorksheetDokument2 SeitenA Secondary Yeast Infection: Student WorksheetJerish Ann AgawinNoch keine Bewertungen
- Anti Mycobacterial DrugsDokument16 SeitenAnti Mycobacterial DrugsIqra NaeemNoch keine Bewertungen
- 300 Word Essay On COVID-19Dokument1 Seite300 Word Essay On COVID-19streetkeykNoch keine Bewertungen
- Prescribing in ChildrenDokument4 SeitenPrescribing in ChildrenArkopal GuptaNoch keine Bewertungen
- Oet SpeakingDokument19 SeitenOet SpeakingChristina DienteNoch keine Bewertungen
- By: Shazleen Farhana Anggun Lestary Advisor: Dr. Diana Muchsin Supervisor: Dr. Asnawi Madjid, SP - KK, MARSDokument25 SeitenBy: Shazleen Farhana Anggun Lestary Advisor: Dr. Diana Muchsin Supervisor: Dr. Asnawi Madjid, SP - KK, MARSShazleen FarhanaNoch keine Bewertungen
- ID-Micro L9 (Atypical Bacteria)Dokument20 SeitenID-Micro L9 (Atypical Bacteria)Oraco1Noch keine Bewertungen
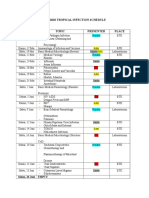
- Imo Tropical Infection ScheduleDokument3 SeitenImo Tropical Infection ScheduleHendroMaleNoch keine Bewertungen