Das könnte Ihnen auch gefallen
- More Instant Self HypnosisDokument66 SeitenMore Instant Self HypnosisSandip Jambhule93% (27)
- Mount Wilga High Level Language Test (Revised) (2006)Dokument78 SeitenMount Wilga High Level Language Test (Revised) (2006)Speech & Language Therapy in Practice75% (8)
- Self AttuneDokument6 SeitenSelf AttuneBodibodi100% (2)
- Circular Questioning As A Therapeutic ToDokument13 SeitenCircular Questioning As A Therapeutic ToNicole Prat CoghlanNoch keine Bewertungen
- EHR Implementation Goals and Objectives GuidelinesDokument12 SeitenEHR Implementation Goals and Objectives GuidelinesrhvenkatNoch keine Bewertungen
- Talking Mats: Speech and Language Research in PracticeDokument4 SeitenTalking Mats: Speech and Language Research in PracticeSpeech & Language Therapy in PracticeNoch keine Bewertungen
- Hearts and Minds HSE RoadmapDokument4 SeitenHearts and Minds HSE RoadmapJorge Valdivia100% (1)
- 360 Process Recording TemplateDokument13 Seiten360 Process Recording Templateapi-252910411100% (9)
- High Performance Work SystemsDokument26 SeitenHigh Performance Work SystemsChristina DcostaNoch keine Bewertungen
- Community Impact ToolkitDokument45 SeitenCommunity Impact ToolkitSarah MenziesNoch keine Bewertungen
- Imprints of The MindDokument5 SeitenImprints of The MindSpeech & Language Therapy in PracticeNoch keine Bewertungen
- Pharmacy MCQSDokument132 SeitenPharmacy MCQSomair zafar100% (6)
- Lost Art of ListeningDokument24 SeitenLost Art of ListeningMardan IulianNoch keine Bewertungen
- In Brief (Spring 11) Dementia and PhonologyDokument1 SeiteIn Brief (Spring 11) Dementia and PhonologySpeech & Language Therapy in PracticeNoch keine Bewertungen
- Strategic Planning in Healthcare: Benefits, Process and ImplementationDokument7 SeitenStrategic Planning in Healthcare: Benefits, Process and Implementationalodia_farichaiNoch keine Bewertungen
- Lymphatic System and San JiaoDokument6 SeitenLymphatic System and San JiaoΒιβιλάκη Γεωργία100% (1)
- Alcool HealthEffectsDokument20 SeitenAlcool HealthEffectsAdrian Stan100% (1)
- Strategic Planning in Healthcare Guides Future FocusDokument10 SeitenStrategic Planning in Healthcare Guides Future Focusim. Elias100% (1)
- OET Reading From U To VDokument12 SeitenOET Reading From U To VLavanya Ranganathan93% (45)
- Turning On The SpotlightDokument6 SeitenTurning On The SpotlightSpeech & Language Therapy in PracticeNoch keine Bewertungen
- The Sullivan Hospital System ReportDokument7 SeitenThe Sullivan Hospital System ReportarvnndNoch keine Bewertungen
- Balanced Scorecard - Chapter 4Dokument21 SeitenBalanced Scorecard - Chapter 4Haseeb AhmedNoch keine Bewertungen
- Strategic Issues in Nonprofit ManagementDokument2 SeitenStrategic Issues in Nonprofit ManagementmythilirajkNoch keine Bewertungen
- CHN Course PlanDokument29 SeitenCHN Course PlanSathya PalanisamyNoch keine Bewertungen
- Four Stages of Planning and Implementation During Covid-19: One Rural Hospital'S Preparations.Dokument14 SeitenFour Stages of Planning and Implementation During Covid-19: One Rural Hospital'S Preparations.Irish ButtNoch keine Bewertungen
- Writing Assignment IIIDokument7 SeitenWriting Assignment IIIAlfredo PanceronNoch keine Bewertungen
- Planning FinalDokument43 SeitenPlanning Finaltownee03Noch keine Bewertungen
- The Balanced Scorecard: Solution at Peel Memorial HospitalDokument4 SeitenThe Balanced Scorecard: Solution at Peel Memorial Hospitaltome44Noch keine Bewertungen
- Guide To Actionable MeasurementDokument21 SeitenGuide To Actionable MeasurementCamaal MotenNoch keine Bewertungen
- Implementing Evidence in Clinical SettingsDokument25 SeitenImplementing Evidence in Clinical SettingsDrmirfat AlkashifNoch keine Bewertungen
- 13 Sample BusinessDokument6 Seiten13 Sample Businessnimisha vermaNoch keine Bewertungen
- IA17A DE160327 CuongHN Lab2Dokument18 SeitenIA17A DE160327 CuongHN Lab2Cường Huỳnh NgọcNoch keine Bewertungen
- Employee Retention WorkbookDokument19 SeitenEmployee Retention WorkbookMOHAMMAD KAWSAR JAHANNoch keine Bewertungen
- Training Needs AssessmentDokument11 SeitenTraining Needs AssessmentIskandar ZulkarnaenNoch keine Bewertungen
- Unit 1Dokument37 SeitenUnit 1Madhu MasihNoch keine Bewertungen
- Rationale of The StudyDokument4 SeitenRationale of The StudyAllysson Mae LicayanNoch keine Bewertungen
- 8 StepsDokument6 Seiten8 StepsAlejandra KimNoch keine Bewertungen
- Work-life integration strategies for organizations and employeesDokument8 SeitenWork-life integration strategies for organizations and employeesmandy02scribdNoch keine Bewertungen
- Subha's Project Repaired)Dokument63 SeitenSubha's Project Repaired)Mehul PanchalNoch keine Bewertungen
- HR ManagementDokument17 SeitenHR ManagementMeenakshi Neelakandan0% (1)
- Transformacion PracticaDokument2 SeitenTransformacion PracticaMario Luna BracamontesNoch keine Bewertungen
- Framework For Ethical Decision-Making: Answer The Following Questions in Your Group. in Each of TheDokument4 SeitenFramework For Ethical Decision-Making: Answer The Following Questions in Your Group. in Each of Theapi-309879220Noch keine Bewertungen
- Chapter 8 - Diagnosis and FeedbackDokument55 SeitenChapter 8 - Diagnosis and FeedbackLeila LibotNoch keine Bewertungen
- Heather Gifford Self-Appraisal2015Dokument2 SeitenHeather Gifford Self-Appraisal2015api-257580555Noch keine Bewertungen
- Performance Improvement (PI) Plan and Template: Health Care Association of New JerseyDokument46 SeitenPerformance Improvement (PI) Plan and Template: Health Care Association of New JerseyRógini HaasNoch keine Bewertungen
- Final Exam HSC 312Dokument5 SeitenFinal Exam HSC 312Milgrid GuzmanNoch keine Bewertungen
- The Characteristics of a High-Performance CultureDokument31 SeitenThe Characteristics of a High-Performance CulturesagarNoch keine Bewertungen
- Module 5 Self-AssessmentDokument4 SeitenModule 5 Self-AssessmentJulie KiselevNoch keine Bewertungen
- A Practical Guide To Using Service User Feedback Outcome ToolsDokument99 SeitenA Practical Guide To Using Service User Feedback Outcome ToolsPeter LawsonNoch keine Bewertungen
- REFOCUS Manual FinalDokument40 SeitenREFOCUS Manual FinalChiriac Andrei TudorNoch keine Bewertungen
- Mission, Vision & PhilosophyDokument40 SeitenMission, Vision & Philosophyamal abdulrahmanNoch keine Bewertungen
- How To Win The Case To Invest in Employee Health and WellbeingDokument4 SeitenHow To Win The Case To Invest in Employee Health and WellbeingKarlNoch keine Bewertungen
- Organizing+ Staffing+ Patient Classification SystemDokument33 SeitenOrganizing+ Staffing+ Patient Classification SystemJek Dela CruzNoch keine Bewertungen
- The Good Indicators Guide:: Understanding How To Use and Choose IndicatorsDokument40 SeitenThe Good Indicators Guide:: Understanding How To Use and Choose IndicatorssuperpaqsNoch keine Bewertungen
- Group DynamicsDokument7 SeitenGroup DynamicsparulpariNoch keine Bewertungen
- scribd.vdownloaders.com_mission-vison-philosophyDokument24 Seitenscribd.vdownloaders.com_mission-vison-philosophyRubina MasihNoch keine Bewertungen
- NCM 119 Lesson 4Dokument119 SeitenNCM 119 Lesson 4Celline Isabelle ReyesNoch keine Bewertungen
- Semester I A Paper OnDokument9 SeitenSemester I A Paper OnAlvin JaymonNoch keine Bewertungen
- Organizational Behavior: 1) How Goal Setting Is Done?Dokument11 SeitenOrganizational Behavior: 1) How Goal Setting Is Done?Sahil VarlaniNoch keine Bewertungen
- Mod 6Dokument13 SeitenMod 6Nikita SangalNoch keine Bewertungen
- Organizational Change and DevelopmentDokument3 SeitenOrganizational Change and DevelopmentSari Marta Krisna IINoch keine Bewertungen
- What's in A Name?Dokument3 SeitenWhat's in A Name?nosheen_noshNoch keine Bewertungen
- Getting Health Reform RightDokument364 SeitenGetting Health Reform RightAmro Peck100% (1)
- Dr. Sherif Eladawy Dr. Amr Bassiouny Dr. Yehia Hussein: Presented byDokument8 SeitenDr. Sherif Eladawy Dr. Amr Bassiouny Dr. Yehia Hussein: Presented byYahya Hassan Hussein El-tamalyNoch keine Bewertungen
- Assessing community strengths and needsDokument3 SeitenAssessing community strengths and needsDarcy Hamada100% (1)
- Organizational Redesign, Restructuring and ReengineeringDokument60 SeitenOrganizational Redesign, Restructuring and ReengineeringJonalynNoch keine Bewertungen
- Which Systems Change Should You Work OnDokument4 SeitenWhich Systems Change Should You Work Onharishpr.internetNoch keine Bewertungen
- IHITool QI Project CharterDokument7 SeitenIHITool QI Project CharterkepheroNoch keine Bewertungen
- Rethinking Nursing Productivity To Enhance Organizational Performance - Final - 2Dokument17 SeitenRethinking Nursing Productivity To Enhance Organizational Performance - Final - 2deepak162162Noch keine Bewertungen
- Employee Welfare Info SheetDokument4 SeitenEmployee Welfare Info SheetJomy JoseNoch keine Bewertungen
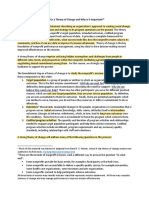
- What Is A Theory of Change and Why Is It Important?: Working Hard and Working WellDokument3 SeitenWhat Is A Theory of Change and Why Is It Important?: Working Hard and Working WellSauharda DhakalNoch keine Bewertungen
- Manage and Maintain Small/Medium Business Operations: Pre. by Jaleto SDokument56 SeitenManage and Maintain Small/Medium Business Operations: Pre. by Jaleto SJaleto sunkemoNoch keine Bewertungen
- Winning Ways (Spring 2008)Dokument1 SeiteWinning Ways (Spring 2008)Speech & Language Therapy in PracticeNoch keine Bewertungen
- Here's One SPR 09 Friendship ThemeDokument1 SeiteHere's One SPR 09 Friendship ThemeSpeech & Language Therapy in PracticeNoch keine Bewertungen
- Winning Ways (Summer 2008)Dokument1 SeiteWinning Ways (Summer 2008)Speech & Language Therapy in PracticeNoch keine Bewertungen
- Here's One I Made Earlier (Spring 2008)Dokument1 SeiteHere's One I Made Earlier (Spring 2008)Speech & Language Therapy in PracticeNoch keine Bewertungen
- In Brief and Critical Friends (Summer 09)Dokument1 SeiteIn Brief and Critical Friends (Summer 09)Speech & Language Therapy in PracticeNoch keine Bewertungen
- Winning Ways (Winter 2007)Dokument1 SeiteWinning Ways (Winter 2007)Speech & Language Therapy in PracticeNoch keine Bewertungen
- In Brief (Spring 09) Speed of SoundDokument1 SeiteIn Brief (Spring 09) Speed of SoundSpeech & Language Therapy in PracticeNoch keine Bewertungen
- Winning Ways (Autumn 2008)Dokument1 SeiteWinning Ways (Autumn 2008)Speech & Language Therapy in PracticeNoch keine Bewertungen
- Here's One Sum 09 Storyteller, Friendship, That's HowDokument1 SeiteHere's One Sum 09 Storyteller, Friendship, That's HowSpeech & Language Therapy in PracticeNoch keine Bewertungen
- In Brief (Spring 10) Acknowledgement, Accessibility, Direct TherapyDokument1 SeiteIn Brief (Spring 10) Acknowledgement, Accessibility, Direct TherapySpeech & Language Therapy in PracticeNoch keine Bewertungen
- Here's One Aut 09 Communication Tree, What On EarthDokument1 SeiteHere's One Aut 09 Communication Tree, What On EarthSpeech & Language Therapy in PracticeNoch keine Bewertungen
- Ylvisaker HandoutDokument20 SeitenYlvisaker HandoutSpeech & Language Therapy in PracticeNoch keine Bewertungen
- In Brief (Summer 11) AphasiaDokument1 SeiteIn Brief (Summer 11) AphasiaSpeech & Language Therapy in PracticeNoch keine Bewertungen
- In Brief (Autumn 09) NQTs and Assessment ClinicsDokument1 SeiteIn Brief (Autumn 09) NQTs and Assessment ClinicsSpeech & Language Therapy in PracticeNoch keine Bewertungen
- In Brief and Here's One Autumn 10Dokument2 SeitenIn Brief and Here's One Autumn 10Speech & Language Therapy in PracticeNoch keine Bewertungen
- In Brief (Summer 10) TeenagersDokument1 SeiteIn Brief (Summer 10) TeenagersSpeech & Language Therapy in PracticeNoch keine Bewertungen
- Here's One Spring 10 Dating ThemeDokument1 SeiteHere's One Spring 10 Dating ThemeSpeech & Language Therapy in PracticeNoch keine Bewertungen
- Here's One I Made Earlier Summer 11Dokument1 SeiteHere's One I Made Earlier Summer 11Speech & Language Therapy in PracticeNoch keine Bewertungen
- Here's One Summer 10Dokument1 SeiteHere's One Summer 10Speech & Language Therapy in PracticeNoch keine Bewertungen
- Here's One Winter 10Dokument1 SeiteHere's One Winter 10Speech & Language Therapy in PracticeNoch keine Bewertungen
- Here's One Spring 11Dokument1 SeiteHere's One Spring 11Speech & Language Therapy in PracticeNoch keine Bewertungen
- In Brief (Winter 10) Stammering and Communication Therapy InternationalDokument2 SeitenIn Brief (Winter 10) Stammering and Communication Therapy InternationalSpeech & Language Therapy in PracticeNoch keine Bewertungen
- Applying Choices and PossibilitiesDokument3 SeitenApplying Choices and PossibilitiesSpeech & Language Therapy in PracticeNoch keine Bewertungen
- Boundary Issues (7) : Drawing The LineDokument1 SeiteBoundary Issues (7) : Drawing The LineSpeech & Language Therapy in PracticeNoch keine Bewertungen
- A Practical FocusDokument2 SeitenA Practical FocusSpeech & Language Therapy in PracticeNoch keine Bewertungen
- Lesson 6 Thyroid and Antithyroid DrugsDokument28 SeitenLesson 6 Thyroid and Antithyroid DrugstheintrovNoch keine Bewertungen
- Australia Evidence Based Management of Acute Musculoskeletal Pain - A Guide For CliniciansDokument84 SeitenAustralia Evidence Based Management of Acute Musculoskeletal Pain - A Guide For CliniciansyohanNoch keine Bewertungen
- Heritage Village ProjectDokument24 SeitenHeritage Village ProjectHaindava Keralam50% (2)
- Investigation, Primary Health Care (PHC)Dokument77 SeitenInvestigation, Primary Health Care (PHC)api-3710926Noch keine Bewertungen
- Scoop of Practice aOTADokument9 SeitenScoop of Practice aOTAfercespedNoch keine Bewertungen
- Langerhans Cell Histiocytosis (LCH) : Guidelines For Diagnosis, Clinical Work-Up, and Treatment For Patients Till The Age of 18 YearsDokument10 SeitenLangerhans Cell Histiocytosis (LCH) : Guidelines For Diagnosis, Clinical Work-Up, and Treatment For Patients Till The Age of 18 Yearsadrian Morales PeraltaNoch keine Bewertungen
- Mood Disorders StudentDokument32 SeitenMood Disorders StudentRafly FernandaNoch keine Bewertungen
- Health Insurance: A Complete Guide in 40 WordsDokument46 SeitenHealth Insurance: A Complete Guide in 40 WordsSandeep KumarNoch keine Bewertungen
- Chapter 48 - Drugs Affecting Blood CoagulationDokument12 SeitenChapter 48 - Drugs Affecting Blood CoagulationJonathon100% (1)
- 6 - B.arun., Safety Positions For Healthy Sex Following Back PainDokument5 Seiten6 - B.arun., Safety Positions For Healthy Sex Following Back PainDr. Krishna N. SharmaNoch keine Bewertungen
- Robbart Van LinschotenDokument234 SeitenRobbart Van LinschotenAtiKa YuLiantiNoch keine Bewertungen
- DKA Protocol With Calculation SheetDokument7 SeitenDKA Protocol With Calculation SheetAmanda Marie Best OsbourneNoch keine Bewertungen
- 02health and DiseaseDokument22 Seiten02health and DiseaseMario GoldingNoch keine Bewertungen
- Gerd NotesDokument14 SeitenGerd NotesNguyen Phuong100% (1)
- Heart Disease Course PDALongDokument84 SeitenHeart Disease Course PDALongArpanpatelNoch keine Bewertungen
- Ventilator Associated PneumoniaDokument2 SeitenVentilator Associated PneumoniaMuzana DariseNoch keine Bewertungen
- User Manual CT PHANTOMS T40016, T40017 andDokument12 SeitenUser Manual CT PHANTOMS T40016, T40017 andAndres AracenaNoch keine Bewertungen
- AbkDokument11 SeitenAbkNurul AiniNoch keine Bewertungen
- HPGD 2103 - Guidance and CounsellingDokument14 SeitenHPGD 2103 - Guidance and CounsellingkhugeshNoch keine Bewertungen
- Impact of Service Quality On Patient Satisfaction A Study at Physiotherapy Unit Pku Muhammadiyah Hospital of YogyakartaDokument5 SeitenImpact of Service Quality On Patient Satisfaction A Study at Physiotherapy Unit Pku Muhammadiyah Hospital of YogyakartaFahmi RizalNoch keine Bewertungen
- Cara Penggunaan Minyak Atsiri OkDokument28 SeitenCara Penggunaan Minyak Atsiri OkYuliNoch keine Bewertungen
- Safe and Sound Protocol Therapeutic TeachingDokument2 SeitenSafe and Sound Protocol Therapeutic TeachingristeacristiNoch keine Bewertungen