Das könnte Ihnen auch gefallen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Scabies and Pediculosis Pubis: An Update of Treatment Regimens and General ReviewDokument7 SeitenScabies and Pediculosis Pubis: An Update of Treatment Regimens and General ReviewNovita WulandariNoch keine Bewertungen
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- NAMA: NIM: : Checklist BLOK 3 Pemeriksaan FisikDokument2 SeitenNAMA: NIM: : Checklist BLOK 3 Pemeriksaan FisikNovita WulandariNoch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Scabies and Pediculosis Pubis: An Update of Treatment Regimens and General ReviewDokument7 SeitenScabies and Pediculosis Pubis: An Update of Treatment Regimens and General ReviewNovita WulandariNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Lion Air - 03 Aug 2014 - YpnoalDokument2 SeitenLion Air - 03 Aug 2014 - YpnoalNovita WulandariNoch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Lecture10animals2 Taxonomy 5Dokument9 SeitenLecture10animals2 Taxonomy 5Novita WulandariNoch keine Bewertungen
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Tuberculosis in Canada: Pre-ReleaseDokument10 SeitenTuberculosis in Canada: Pre-ReleaseNovita WulandariNoch keine Bewertungen
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Cerebral Blood Flow by Arterial Spin Labeling in Poststroke DementiaDokument7 SeitenCerebral Blood Flow by Arterial Spin Labeling in Poststroke DementiaNovita WulandariNoch keine Bewertungen
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- 996 FullDokument9 Seiten996 FullNovita WulandariNoch keine Bewertungen
- Spinal Anaesthesia A Practical GuideDokument14 SeitenSpinal Anaesthesia A Practical GuideNovita WulandariNoch keine Bewertungen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Form Konfirmasi Sponsorship (Hoka Hoka Bento)Dokument1 SeiteForm Konfirmasi Sponsorship (Hoka Hoka Bento)Novita WulandariNoch keine Bewertungen
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Intratympanic Bupivacaine Instillation For Tinnitus Treatment?Dokument4 SeitenIntratympanic Bupivacaine Instillation For Tinnitus Treatment?Novita WulandariNoch keine Bewertungen
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Social Isolation Affects The Development of Obesity and Type 2 Diabetes in MiceDokument9 SeitenSocial Isolation Affects The Development of Obesity and Type 2 Diabetes in MiceNovita WulandariNoch keine Bewertungen
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Spinal Anaesthesia A Practical GuideDokument14 SeitenSpinal Anaesthesia A Practical GuideNovita WulandariNoch keine Bewertungen
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- Blood Pressure Management in Patients With Diabetes: Clinical Trial Evidence For BP ControlDokument8 SeitenBlood Pressure Management in Patients With Diabetes: Clinical Trial Evidence For BP ControlNovita WulandariNoch keine Bewertungen
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Canfamphys00278 0097Dokument2 SeitenCanfamphys00278 0097Novita WulandariNoch keine Bewertungen
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Efavirenz Chem OlympicsDokument1 SeiteEfavirenz Chem OlympicsdreamingsnowNoch keine Bewertungen
- PHD Thesis On Medical Tourism in IndiaDokument4 SeitenPHD Thesis On Medical Tourism in IndiaBuyingCollegePapersPittsburgh100% (1)
- What Is Alzheimer's - Alzheimer's AssociationDokument6 SeitenWhat Is Alzheimer's - Alzheimer's AssociationRatnaPrasadNalamNoch keine Bewertungen
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Pelvic Organ ProlapseDokument9 SeitenPelvic Organ ProlapseSonny Dizon PareñasNoch keine Bewertungen
- Lab 1 - Asepsis and Infection Control QuestionsDokument3 SeitenLab 1 - Asepsis and Infection Control QuestionsmlomiguenNoch keine Bewertungen
- The Learning Curve For Laparoscopic Cholecystectomy PDFDokument5 SeitenThe Learning Curve For Laparoscopic Cholecystectomy PDFIgor CemortanNoch keine Bewertungen
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Healthcare Hospital MaintenanceDokument302 SeitenHealthcare Hospital Maintenanceshahar397100% (2)
- Oxaliplatin Monograph 1dec2016Dokument9 SeitenOxaliplatin Monograph 1dec2016Nadial UzmahNoch keine Bewertungen
- Foods That Can Purify Blood Naturally - PositiveMedffDokument7 SeitenFoods That Can Purify Blood Naturally - PositiveMedfftmk1989Noch keine Bewertungen
- Sample Size PilotDokument5 SeitenSample Size PilotmsriramcaNoch keine Bewertungen
- Doxazosin Mesilate - Martindale 36edDokument1 SeiteDoxazosin Mesilate - Martindale 36edSvetlana Maiochi LodovicoNoch keine Bewertungen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- The Guide To The Future of Medicine White PaperDokument25 SeitenThe Guide To The Future of Medicine White PaperJose Avila100% (4)
- Nutritional Benefits: This Parcel of Vegetable Is Nutrient-Packed and Low in Calorie. It IsDokument10 SeitenNutritional Benefits: This Parcel of Vegetable Is Nutrient-Packed and Low in Calorie. It IsEdel MartinezNoch keine Bewertungen
- Drug Study For HELLP SyndromeDokument19 SeitenDrug Study For HELLP SyndromeRosemarie CarpioNoch keine Bewertungen
- 14 Exercises For Shoulder Pain Relief & Rehab (Printable PDFDokument19 Seiten14 Exercises For Shoulder Pain Relief & Rehab (Printable PDFlalita100% (1)
- TCCC Quick Reference Guide 2017Dokument54 SeitenTCCC Quick Reference Guide 2017https://www.t-medical.orgNoch keine Bewertungen
- Consciousness PsychologyDokument32 SeitenConsciousness PsychologyDeea Addine As-SoubNoch keine Bewertungen
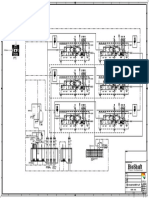
- P&ID - STP-Yanbu SWCC (6units)Dokument1 SeiteP&ID - STP-Yanbu SWCC (6units)Ashraf BayomiNoch keine Bewertungen
- Which of The Following Complications Is Thought To Be The Most Common Cause of AppendicitisDokument15 SeitenWhich of The Following Complications Is Thought To Be The Most Common Cause of AppendicitisKristine CastilloNoch keine Bewertungen
- LIST OF REGISTERED DRUGS As of December 2012: DR No Generic Brand Strength Form CompanyDokument33 SeitenLIST OF REGISTERED DRUGS As of December 2012: DR No Generic Brand Strength Form CompanyBenjamin Tantiansu50% (2)
- Intra Uterine Insemination - IUIDokument15 SeitenIntra Uterine Insemination - IUIlayyous100% (1)
- Ways of Enhancing Pulp Preservation by Stepwise Excavation-A Systematic Review PDFDokument13 SeitenWays of Enhancing Pulp Preservation by Stepwise Excavation-A Systematic Review PDFFabian ArangoNoch keine Bewertungen
- Benefits of Zinc:: 1 - Zinc and Regulating Immune FunctionDokument3 SeitenBenefits of Zinc:: 1 - Zinc and Regulating Immune FunctionHuda BaharoonNoch keine Bewertungen
- FNB-Minimal Access Surgery: Competency Based Training ProgrammeDokument31 SeitenFNB-Minimal Access Surgery: Competency Based Training ProgrammeAMBUJ KUMAR SONINoch keine Bewertungen
- Current Evidence For The Management of Schizoaffective DisorderDokument12 SeitenCurrent Evidence For The Management of Schizoaffective DisorderabdulNoch keine Bewertungen
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- South West Regional Bulletin: A Message From The Director All Change at The CentreDokument19 SeitenSouth West Regional Bulletin: A Message From The Director All Change at The Centre433188Noch keine Bewertungen
- 29a ΙΡΙΔΟΛΟΓΙΑ EGDokument28 Seiten29a ΙΡΙΔΟΛΟΓΙΑ EGO TΣΑΡΟΣ ΤΗΣ ΑΝΤΙΒΑΡΥΤΗΤΑΣ ΛΙΑΠΗΣ ΠΑΝΑΓΙΩΤΗΣNoch keine Bewertungen
- Liposomal Drug Delivery SystemDokument15 SeitenLiposomal Drug Delivery SystemsyeedNoch keine Bewertungen
- New Prescription For Drug Makers - Update The Plants - WSJDokument5 SeitenNew Prescription For Drug Makers - Update The Plants - WSJStacy Kelly100% (1)
- Dispelling Myths About Drinking Distilled WaterDokument6 SeitenDispelling Myths About Drinking Distilled WaterPau StraitNoch keine Bewertungen
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Von EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Bewertung: 3 von 5 Sternen3/5 (1)