Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Tline Poinsettia Tracker PDFDokument1 SeiteTline Poinsettia Tracker PDFKolekade-Mattandkira AckerNoch keine Bewertungen
- Tline Poinsettia TrackerDokument1 SeiteTline Poinsettia TrackerKolekade-Mattandkira AckerNoch keine Bewertungen
- Tline Anaerobic Endurance Training PDFDokument1 SeiteTline Anaerobic Endurance Training PDFKolekade-Mattandkira AckerNoch keine Bewertungen
- TLine PoinsettiasDokument1 SeiteTLine PoinsettiasKolekade-Mattandkira AckerNoch keine Bewertungen
- Tline Warm-Up, Cool-Down and Flexibility PDFDokument1 SeiteTline Warm-Up, Cool-Down and Flexibility PDFKolekade-Mattandkira AckerNoch keine Bewertungen
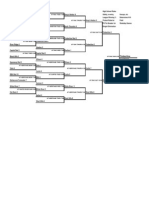
- JV BracketDokument1 SeiteJV BracketKolekade-Mattandkira AckerNoch keine Bewertungen
- Tline In-Season Pitching PDFDokument1 SeiteTline In-Season Pitching PDFKolekade-Mattandkira AckerNoch keine Bewertungen
- Tline Training Periodizaton Schedule PDFDokument2 SeitenTline Training Periodizaton Schedule PDFKolekade-Mattandkira AckerNoch keine Bewertungen
- Tline Feet-to-Fingertips Weight Training PDFDokument1 SeiteTline Feet-to-Fingertips Weight Training PDFKolekade-Mattandkira AckerNoch keine Bewertungen
- Tline Pitcing Program PDFDokument6 SeitenTline Pitcing Program PDFKolekade-Mattandkira AckerNoch keine Bewertungen
- Thurston County Baseball PDFDokument1 SeiteThurston County Baseball PDFKolekade-Mattandkira AckerNoch keine Bewertungen
- Tline Strenght and Power Training PDFDokument9 SeitenTline Strenght and Power Training PDFKolekade-Mattandkira AckerNoch keine Bewertungen
- PS Fall Ball Standings 2013Dokument1 SeitePS Fall Ball Standings 2013Kolekade-Mattandkira AckerNoch keine Bewertungen
- Varsity BracketDokument3 SeitenVarsity BracketKolekade-Mattandkira AckerNoch keine Bewertungen
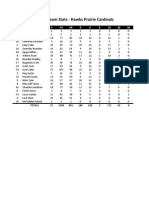
- Cards Hitting 2013Dokument2 SeitenCards Hitting 2013Kolekade-Mattandkira AckerNoch keine Bewertungen
- PS Fall Ball Schedule 2013Dokument1 SeitePS Fall Ball Schedule 2013Kolekade-Mattandkira AckerNoch keine Bewertungen
- Cards Pitching 2013Dokument2 SeitenCards Pitching 2013Kolekade-Mattandkira AckerNoch keine Bewertungen
- PSCL Hawaii Camp FormDokument1 SeitePSCL Hawaii Camp FormKolekade-Mattandkira AckerNoch keine Bewertungen
- Silvers Hitting 2013Dokument2 SeitenSilvers Hitting 2013Kolekade-Mattandkira AckerNoch keine Bewertungen
- Silvers Pitching 2013Dokument2 SeitenSilvers Pitching 2013Kolekade-Mattandkira AckerNoch keine Bewertungen
- Saints Hitting 2013Dokument2 SeitenSaints Hitting 2013Kolekade-Mattandkira AckerNoch keine Bewertungen
- A's Hitting 2013Dokument2 SeitenA's Hitting 2013Kolekade-Mattandkira AckerNoch keine Bewertungen
- Brewers Pitching 2013Dokument2 SeitenBrewers Pitching 2013Kolekade-Mattandkira AckerNoch keine Bewertungen
- A's Pitching 2013Dokument2 SeitenA's Pitching 2013Kolekade-Mattandkira AckerNoch keine Bewertungen
- Brewers Hitting 2013Dokument2 SeitenBrewers Hitting 2013Kolekade-Mattandkira AckerNoch keine Bewertungen
- Fathers Day Umpire Schedule 2013Dokument2 SeitenFathers Day Umpire Schedule 2013Kolekade-Mattandkira AckerNoch keine Bewertungen
- Saints Pitching 2013Dokument2 SeitenSaints Pitching 2013Kolekade-Mattandkira AckerNoch keine Bewertungen
- Linx Hitting 2013Dokument2 SeitenLinx Hitting 2013Kolekade-Mattandkira AckerNoch keine Bewertungen
- Linx Pitching 2013Dokument2 SeitenLinx Pitching 2013Kolekade-Mattandkira AckerNoch keine Bewertungen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- This Study Resource Was: Patient InformationDokument1 SeiteThis Study Resource Was: Patient InformationissaiahnicolleNoch keine Bewertungen
- Homeopathic Materia Medica of Apis by Allen S HandbookDokument13 SeitenHomeopathic Materia Medica of Apis by Allen S HandbookaldodiasNoch keine Bewertungen
- Catalogo SomsoDokument160 SeitenCatalogo SomsoAlejandro TabiloskyNoch keine Bewertungen
- Reinterpreting Ba Duan Jing From The Theories of The Eight Extra MeridiansDokument20 SeitenReinterpreting Ba Duan Jing From The Theories of The Eight Extra MeridiansAdrian Stan100% (1)
- Kapalabhati Pranayama or Breath of FireDokument6 SeitenKapalabhati Pranayama or Breath of Firemsayee100% (1)
- Bubble He Assessment: Vital SignsDokument11 SeitenBubble He Assessment: Vital SignsFregen Mae ApoyaNoch keine Bewertungen
- Bsn3-2c UC-BCF CVA Case StudyDokument49 SeitenBsn3-2c UC-BCF CVA Case StudyclarheenaNoch keine Bewertungen
- Chi Nei Tsang IDokument9 SeitenChi Nei Tsang Ijuanitos111Noch keine Bewertungen
- The Lung Meridian Acu-PointsDokument1 SeiteThe Lung Meridian Acu-PointsVicaas VSNoch keine Bewertungen
- Respiratory EmergenciesDokument30 SeitenRespiratory EmergenciesNovriefta NugrahaNoch keine Bewertungen
- Top 5 Acupressure Points To Treat Cold, Flu and FeverDokument16 SeitenTop 5 Acupressure Points To Treat Cold, Flu and Feverdlpurpos0% (1)
- Study Questions for Part II Thoracic SurgeryDokument15 SeitenStudy Questions for Part II Thoracic SurgeryIbrahim Barham50% (2)
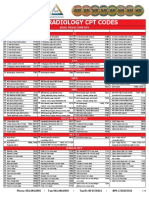
- 2019 Radiology CPT Codes: CT Bone DensitometryDokument2 Seiten2019 Radiology CPT Codes: CT Bone DensitometryDownsyndrome CyborgNoch keine Bewertungen
- History Taking and PEDokument30 SeitenHistory Taking and PEMelissa Salayog100% (1)
- A Practical Gdfguide To Conscious Out of Body ExperiencesDokument17 SeitenA Practical Gdfguide To Conscious Out of Body ExperiencesHandrew FPVNoch keine Bewertungen
- Public SpeakingDokument313 SeitenPublic Speakingabhishekchit100% (1)
- Scan 17-Nov-2021Dokument6 SeitenScan 17-Nov-2021Savita AgrawalNoch keine Bewertungen
- Exercises and Yoga For Cervical Spondylosis: Neck PainDokument5 SeitenExercises and Yoga For Cervical Spondylosis: Neck PainKaran Aggarwal100% (2)
- MRCS Part A 10 Jan 2017 Recalls (DR Salah Group) .Dokument7 SeitenMRCS Part A 10 Jan 2017 Recalls (DR Salah Group) .Umair Ashfaq0% (1)
- Instant Download Ebook PDF Essentials of Athletic Injury Management 10th Edition PDF ScribdDokument41 SeitenInstant Download Ebook PDF Essentials of Athletic Injury Management 10th Edition PDF Scribdjune.thompson131100% (40)
- 18 Yoga BabajiDokument31 Seiten18 Yoga BabajiSubramanya Seshagiri100% (1)
- Icpm V2 PDFDokument169 SeitenIcpm V2 PDFKannan SNoch keine Bewertungen
- Pear Cone WaveDokument2 SeitenPear Cone WaveMichael Grant White100% (2)
- Thorax and LungsDokument3 SeitenThorax and LungsJL RebeseNoch keine Bewertungen
- ANAPHY Respiratory SystemDokument30 SeitenANAPHY Respiratory SystemAshley Franceska CansanayNoch keine Bewertungen
- Chicken Anatomy & PhysiologyDokument26 SeitenChicken Anatomy & PhysiologySanjeev ChaudharyNoch keine Bewertungen
- Case Study (Acute Pyelonephritis) FINALDokument20 SeitenCase Study (Acute Pyelonephritis) FINALian-movilla-751780% (10)
- 0fcfcc PDFDokument288 Seiten0fcfcc PDFDick Jonhnson100% (2)
- Step 2. Check For Unresponsiveness-Simultaneously Check For BreathingDokument4 SeitenStep 2. Check For Unresponsiveness-Simultaneously Check For BreathingIvy Jorene Roman RodriguezNoch keine Bewertungen
- Flail Chest (Tayug)Dokument25 SeitenFlail Chest (Tayug)Adrian MallarNoch keine Bewertungen