Das könnte Ihnen auch gefallen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5795)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- Constipation: Practice GapsDokument16 SeitenConstipation: Practice GapsMafer LealNoch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Visual PathwayDokument36 SeitenVisual PathwayVishakh Isloor100% (1)
- Poster 10 PALS 01 01 ENG V20100927 PDFDokument1 SeitePoster 10 PALS 01 01 ENG V20100927 PDFAndy XiaoNoch keine Bewertungen
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Arnett - Soft Tissue Cephalometric AnalysisDokument15 SeitenArnett - Soft Tissue Cephalometric AnalysisVicente Contreras100% (1)
- An Allis Is Used To Grasp Tissue. Available in Short and Long Sizes. A "Judd-Allis" Holds Intestinal Tissue A "Heavy Allis" Holds Breast TissueDokument26 SeitenAn Allis Is Used To Grasp Tissue. Available in Short and Long Sizes. A "Judd-Allis" Holds Intestinal Tissue A "Heavy Allis" Holds Breast TissueSheelah D. TilloNoch keine Bewertungen
- Anatomy MCQDokument23 SeitenAnatomy MCQPirabakar Mahendran100% (3)
- Developmental Assessment of Hospitalized ChildDokument11 SeitenDevelopmental Assessment of Hospitalized ChildmcowellNoch keine Bewertungen
- Health6 q1 Mod5 Community Health Resources and Facilities v2Dokument21 SeitenHealth6 q1 Mod5 Community Health Resources and Facilities v2Bryle Castro100% (3)
- 12 Finishing and DetailingDokument92 Seiten12 Finishing and Detailingtanmayi minniNoch keine Bewertungen
- Blueprints Orthopedics by Grant CooperDokument20 SeitenBlueprints Orthopedics by Grant CooperLucian Husdup20% (5)
- Fluid Management - Presentation PDFDokument16 SeitenFluid Management - Presentation PDFjuniorebinda100% (1)
- Labor Analgesia An UpdateDokument86 SeitenLabor Analgesia An UpdateFarkhan Putra IINoch keine Bewertungen
- Acr Technical Standard For Diagnostic Medical Physics Performance Monitoring of Magnetic Resonance Imaging (Mri) EquipmentDokument4 SeitenAcr Technical Standard For Diagnostic Medical Physics Performance Monitoring of Magnetic Resonance Imaging (Mri) EquipmentFarkhan Putra IINoch keine Bewertungen
- MRI WristDokument14 SeitenMRI WristFarkhan Putra IINoch keine Bewertungen
- Lightning and Its Association With The Frequency of Headache in Migraineurs: An Observational Cohort StudyDokument9 SeitenLightning and Its Association With The Frequency of Headache in Migraineurs: An Observational Cohort StudyFarkhan Putra IINoch keine Bewertungen
- Anterior-Posterior Chest Exam PhotoguideDokument9 SeitenAnterior-Posterior Chest Exam PhotoguideMark GuirguisNoch keine Bewertungen
- Credentials and Privileging of Doctor and NursesDokument56 SeitenCredentials and Privileging of Doctor and NursesManoj KumarNoch keine Bewertungen
- HaryanaDokument15 SeitenHaryanaStudy with meNoch keine Bewertungen
- Personal Profile: Al Mallah AliDokument2 SeitenPersonal Profile: Al Mallah AliAli MallahNoch keine Bewertungen
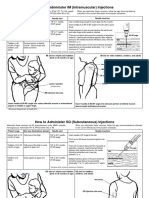
- Im SQ Admin PDFDokument2 SeitenIm SQ Admin PDFAlvin JjNoch keine Bewertungen
- Glossary EyeDokument228 SeitenGlossary EyeCarolus AugustusNoch keine Bewertungen
- Conjoined Twins: Bioethics, Medicine and The Law: ViewpointDokument2 SeitenConjoined Twins: Bioethics, Medicine and The Law: ViewpointSulistyawati WrimunNoch keine Bewertungen
- Intermediate MSUD: Maple Syrup Urine Disease (MSUD)Dokument1 SeiteIntermediate MSUD: Maple Syrup Urine Disease (MSUD)Awais_123Noch keine Bewertungen
- Nail Clubbing - Wikipedia, The Free EncyclopediaDokument4 SeitenNail Clubbing - Wikipedia, The Free EncyclopediaRizalyose SibulNoch keine Bewertungen
- CMS Neuro Form Number 4 Query Answer Req? - USMLE Forum: Jun 30, 2016 - 7 PostsDokument3 SeitenCMS Neuro Form Number 4 Query Answer Req? - USMLE Forum: Jun 30, 2016 - 7 Postsbob0% (1)
- Otitis MediaDokument7 SeitenOtitis MediaNorminaKiramAkmadNoch keine Bewertungen
- Poliomyelitis Disease Investigation GuidelineDokument11 SeitenPoliomyelitis Disease Investigation Guidelineaikohama89Noch keine Bewertungen
- IJRID1063Dokument4 SeitenIJRID1063Wulan Rambitan100% (1)
- LeptospirosisDokument2 SeitenLeptospirosisGurungSurajNoch keine Bewertungen
- Surgical Instruments 3Dokument110 SeitenSurgical Instruments 3Gerald Resubal OriñaNoch keine Bewertungen
- Coeliac Disease: John S. Leeds, Andrew D. Hopper, and David S. SandersDokument14 SeitenCoeliac Disease: John S. Leeds, Andrew D. Hopper, and David S. Sandersbdalcin5512Noch keine Bewertungen
- Sample Thesis Medical Surgical NursingDokument5 SeitenSample Thesis Medical Surgical Nursingafcnuaacq100% (2)
- Neuromuscular Junction by Dr. RoomiDokument20 SeitenNeuromuscular Junction by Dr. RoomiMudassar Roomi100% (1)
- Invitation OSCE PEP Workshop 23rd Juley 2020Dokument1 SeiteInvitation OSCE PEP Workshop 23rd Juley 2020akshayajainaNoch keine Bewertungen