Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Physical Assessment Guide of Head-To-ToeDokument9 SeitenPhysical Assessment Guide of Head-To-Toeneleh gray100% (2)
- Fundamentals of NursingDokument3 SeitenFundamentals of Nursingneleh grayNoch keine Bewertungen
- NR 325 Neuro Worksheet 2Dokument6 SeitenNR 325 Neuro Worksheet 2John Thomas100% (1)
- Glossary of Immune System TermsDokument5 SeitenGlossary of Immune System Termsneleh grayNoch keine Bewertungen
- Fluid & Electrolyte Imbalance/ DehydrationDokument7 SeitenFluid & Electrolyte Imbalance/ Dehydrationneleh grayNoch keine Bewertungen
- ncm105 /mental HealthDokument8 Seitenncm105 /mental Healthneleh grayNoch keine Bewertungen
- Fluid & Electrolyte Imbalance/ DehydrationDokument7 SeitenFluid & Electrolyte Imbalance/ Dehydrationneleh grayNoch keine Bewertungen
- Key Areas of ResponsibilityDokument2 SeitenKey Areas of Responsibilityneleh grayNoch keine Bewertungen
- Vital Signs TableDokument5 SeitenVital Signs Tableneleh grayNoch keine Bewertungen
- Blood Supply of The BrainDokument11 SeitenBlood Supply of The Brainneleh grayNoch keine Bewertungen
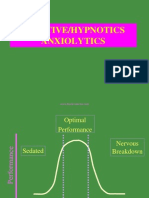
- An Xy Olitics HypnoticsDokument59 SeitenAn Xy Olitics Hypnoticsneleh grayNoch keine Bewertungen
- Anxiolytic DrugsDokument60 SeitenAnxiolytic Drugsneleh grayNoch keine Bewertungen
- Rib, Fractures: Background: Thoracic Trauma Often Involves Multiple Organ Systems and Several AnatomicDokument24 SeitenRib, Fractures: Background: Thoracic Trauma Often Involves Multiple Organ Systems and Several Anatomicneleh grayNoch keine Bewertungen
- Fundamentals of Nursing NotesDokument11 SeitenFundamentals of Nursing Notesneleh grayNoch keine Bewertungen
- Feeding Via Gastric GavageDokument3 SeitenFeeding Via Gastric Gavageneleh gray0% (1)
- Feeding Via Gastric GavageDokument3 SeitenFeeding Via Gastric Gavageneleh gray0% (1)
- Broken Rib SymptomsDokument12 SeitenBroken Rib Symptomsneleh grayNoch keine Bewertungen
- Parotid GlandDokument2 SeitenParotid Glandneleh grayNoch keine Bewertungen
- Fundamentals of NursingDokument12 SeitenFundamentals of Nursingneleh grayNoch keine Bewertungen
- Fundamentals of NursingDokument12 SeitenFundamentals of Nursingneleh grayNoch keine Bewertungen
- Stages of Labor Nursing ConsiderationsDokument5 SeitenStages of Labor Nursing Considerationsneleh gray100% (2)
- Abortion CaseDokument41 SeitenAbortion Casekaycee_delacruz60% (5)
- Neurotransmitters Implicated in Psychiatry: MENTOR-Dr. Lokesh Shekhawat Sir. PRESENTOR - Dr. Vibha TomarDokument79 SeitenNeurotransmitters Implicated in Psychiatry: MENTOR-Dr. Lokesh Shekhawat Sir. PRESENTOR - Dr. Vibha Tomaranon_870875350100% (1)
- Atypical Parkinsonian Disorders: Eugene C. Lai, M.D., PH.DDokument39 SeitenAtypical Parkinsonian Disorders: Eugene C. Lai, M.D., PH.DAssolaSaadNoch keine Bewertungen
- Anti Parkinson Drugs FinallDokument36 SeitenAnti Parkinson Drugs FinallandrapradeshsseNoch keine Bewertungen
- NeurophysiologyDokument72 SeitenNeurophysiologyRaihan LuthfiNoch keine Bewertungen
- ParkinsonDokument2 SeitenParkinsongoyaNoch keine Bewertungen
- Exercise For ParkinsonDokument4 SeitenExercise For Parkinsondefri rahmanNoch keine Bewertungen
- Pyramid & Extrapyramidal DisordersDokument5 SeitenPyramid & Extrapyramidal Disordersjoelh9Noch keine Bewertungen
- OSCE S BibleDokument66 SeitenOSCE S BibleApoorva SaxenaNoch keine Bewertungen
- Print Report Part BDokument82 SeitenPrint Report Part BArun PrasadNoch keine Bewertungen
- Parkinson'S Diseases (PD) : by Dr. Rommanah Azmi PM 013/09Dokument17 SeitenParkinson'S Diseases (PD) : by Dr. Rommanah Azmi PM 013/09Rommanah AzmiNoch keine Bewertungen
- Differential Diagnosis of ParkinsonismDokument27 SeitenDifferential Diagnosis of Parkinsonismelenac67Noch keine Bewertungen
- A Neurocognitive Perspective On Language: The Declarative/ Procedural ModelDokument11 SeitenA Neurocognitive Perspective On Language: The Declarative/ Procedural Models0453737Noch keine Bewertungen
- Prevention For Neuromuscular Conditions: Brig (R) Ali Nasre AlamDokument26 SeitenPrevention For Neuromuscular Conditions: Brig (R) Ali Nasre AlamShimmering Moon100% (1)
- Parkinson's Disease-Diagnosis & TreatmentDokument9 SeitenParkinson's Disease-Diagnosis & Treatmentvivek_win95100% (1)
- Parkinson's Article - PDF 66666666666Dokument11 SeitenParkinson's Article - PDF 66666666666kavyasumanaNoch keine Bewertungen
- Hyperkinetic Movement DisordersDokument209 SeitenHyperkinetic Movement DisordersRaluca-Andreea Ignat100% (1)
- Parkinson's Disease - WikipediaDokument37 SeitenParkinson's Disease - WikipediaAvani ThakkarNoch keine Bewertungen
- Neuroanatomy MCQDokument7 SeitenNeuroanatomy MCQi can always make u smile :D78% (9)
- Parkinson Professional GuideDokument172 SeitenParkinson Professional GuideGibran Ilham100% (2)
- Parkinson DiseaseDokument3 SeitenParkinson DiseaseBen Asiel PadangNoch keine Bewertungen
- KNGF Guideline For Physical Therapy in Patients With ParkinsDokument89 SeitenKNGF Guideline For Physical Therapy in Patients With ParkinsSrđan ŠarenacNoch keine Bewertungen
- Diagnosis For ParkinsonDokument7 SeitenDiagnosis For ParkinsonAnna Mae SuminguitNoch keine Bewertungen
- Parkinson's DiseaseDokument23 SeitenParkinson's DiseaseMonika Joseph100% (2)
- Neuro MCQDokument15 SeitenNeuro MCQSushanta BhanjaNoch keine Bewertungen
- AUJ Analysis and Implementation of Machine Learning Model For Detection of Parkinsons DiseaseDokument8 SeitenAUJ Analysis and Implementation of Machine Learning Model For Detection of Parkinsons DiseaseMohan DehuryNoch keine Bewertungen
- Neurosensory Disorders 22306Dokument14 SeitenNeurosensory Disorders 22306bekbekk cabahugNoch keine Bewertungen
- Extrapyramidal System and CerebellumDokument31 SeitenExtrapyramidal System and CerebellumDanielMahendraNoch keine Bewertungen
- Parkinson'S Disease: by - Nikita Borade BPT Final YearDokument42 SeitenParkinson'S Disease: by - Nikita Borade BPT Final YearNikks BoradeNoch keine Bewertungen
- Case Study 2FDokument2 SeitenCase Study 2Foumou80Noch keine Bewertungen