Das könnte Ihnen auch gefallen
- Vitamins and Minerals 09 V 2Dokument42 SeitenVitamins and Minerals 09 V 2giannidietNoch keine Bewertungen
- Vegetarian Diet-Panacea For Modern Lifestyle DiseasesDokument14 SeitenVegetarian Diet-Panacea For Modern Lifestyle DiseasesgiannidietNoch keine Bewertungen
- Studi Scient RugbyDokument6 SeitenStudi Scient RugbygiannidietNoch keine Bewertungen
- Soccer Sports Nutrition Presentation U11 U14Dokument11 SeitenSoccer Sports Nutrition Presentation U11 U14giannidietNoch keine Bewertungen
- GSSI Carbs Hormones EndDokument5 SeitenGSSI Carbs Hormones EndgiannidietNoch keine Bewertungen
- EFSA - 2010 - Stevia GRASSDokument84 SeitenEFSA - 2010 - Stevia GRASSLiliana CelayaNoch keine Bewertungen
- Eating in The ZoneDokument7 SeitenEating in The ZonejafrinkNoch keine Bewertungen
- Brain FuelDokument2 SeitenBrain FuelgiannidietNoch keine Bewertungen
- Training RecoveryDokument23 SeitenTraining Recoveryapi-3835136100% (1)
- Energy Density of Foods, But Not Beverages, Is Positively Associated With Body Mass Index in Adult WomenDokument8 SeitenEnergy Density of Foods, But Not Beverages, Is Positively Associated With Body Mass Index in Adult WomengiannidietNoch keine Bewertungen
- Session5E-SixWaystoBuildStamina - ManageFatigueDokument4 SeitenSession5E-SixWaystoBuildStamina - ManageFatiguegiannidiet100% (1)
- Carbohydrate Ingestion Can Completely Suppress Endogenous Glucose Production During ExerciseDokument13 SeitenCarbohydrate Ingestion Can Completely Suppress Endogenous Glucose Production During ExercisegiannidietNoch keine Bewertungen
- Salt Intake, Stroke, and Cardiovascular Disease Meta-Analysis of Prospective StudiesDokument9 SeitenSalt Intake, Stroke, and Cardiovascular Disease Meta-Analysis of Prospective StudiesPatrícia BentoNoch keine Bewertungen
- Scientific Abstracts About Dairy and HealthDokument5 SeitenScientific Abstracts About Dairy and HealthgiannidietNoch keine Bewertungen
- 12weeks WomenDokument49 Seiten12weeks Womenusmanmughal111100% (5)
- Whole-Body Skeletal Muscle MassDokument7 SeitenWhole-Body Skeletal Muscle MassgiannidietNoch keine Bewertungen
- International Journal Sports NutritionDokument13 SeitenInternational Journal Sports NutritiongiannidietNoch keine Bewertungen
- Cism08 Sports DieteticsDokument12 SeitenCism08 Sports DieteticsgiannidietNoch keine Bewertungen
- The Cut DietDokument76 SeitenThe Cut DietMarc David83% (6)
- GSSI-High Carbohydrate Meals and PerformanceDokument8 SeitenGSSI-High Carbohydrate Meals and PerformancegiannidietNoch keine Bewertungen
- Sports Nutrition For Young Adults: HydrationDokument4 SeitenSports Nutrition For Young Adults: HydrationgiannidietNoch keine Bewertungen
- Medium Chain TriglyceridesDokument3 SeitenMedium Chain TriglyceridesgiannidietNoch keine Bewertungen
- Early Postexercise Muscle Glycogen Recovery IsDokument9 SeitenEarly Postexercise Muscle Glycogen Recovery IsgiannidietNoch keine Bewertungen
- Martial Arts News and Report: Women's DefenseDokument4 SeitenMartial Arts News and Report: Women's DefensegiannidietNoch keine Bewertungen
- Game DayDokument20 SeitenGame Daygiannidiet100% (1)
- The 7th Workshop On The Assessment of Adequate Intake of Dietary Amino Acids-Summary of General DiscussionDokument3 SeitenThe 7th Workshop On The Assessment of Adequate Intake of Dietary Amino Acids-Summary of General DiscussiongiannidietNoch keine Bewertungen
- Talbott CV 2008Dokument4 SeitenTalbott CV 2008giannidietNoch keine Bewertungen
- Omics of Nutrition A New ParadigmDokument7 SeitenOmics of Nutrition A New ParadigmgiannidietNoch keine Bewertungen
- Multivitamin Use and Telomere Length in WomenDokument7 SeitenMultivitamin Use and Telomere Length in WomengiannidietNoch keine Bewertungen
- Dados-Artigos-Nutricao-Nutricao Esportiva e Suplementacao-Supplementation of L-Carnitine in AthletesDokument7 SeitenDados-Artigos-Nutricao-Nutricao Esportiva e Suplementacao-Supplementation of L-Carnitine in AthletesSri Nowo MinartiNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- FIFA ScripDokument92 SeitenFIFA ScripAlin PoiataNoch keine Bewertungen
- Classification of Techniques in Kodokan Jud1Dokument2 SeitenClassification of Techniques in Kodokan Jud1asgharm10Noch keine Bewertungen
- MATHEMATICS TEST 2Dokument10 SeitenMATHEMATICS TEST 2deyaa1000000Noch keine Bewertungen
- System OffensesDokument3 SeitenSystem OffensesJerad BixlerNoch keine Bewertungen
- Sports - Illustrated.kids March.2022Dokument58 SeitenSports - Illustrated.kids March.2022Belu IonNoch keine Bewertungen
- Vintage Airplane - Oct 1990Dokument40 SeitenVintage Airplane - Oct 1990Aviation/Space History LibraryNoch keine Bewertungen
- Virender Sehwag: Help InfoDokument2 SeitenVirender Sehwag: Help Infovaisakh777Noch keine Bewertungen
- Volleyball U-17 Boys 2023-24Dokument1 SeiteVolleyball U-17 Boys 2023-24Ayushmaan MaithaniNoch keine Bewertungen
- Tactics Time Newsletters. Vol.3 Chess Tactics From The Real Games of Everyday Chess PlayersDokument312 SeitenTactics Time Newsletters. Vol.3 Chess Tactics From The Real Games of Everyday Chess PlayersAbdullah Muceddidi100% (1)
- Krista Hack ResumeDokument4 SeitenKrista Hack Resumeapi-389269145Noch keine Bewertungen
- Chess Handbook For Parents and Coaches: Ronn MunstermanDokument29 SeitenChess Handbook For Parents and Coaches: Ronn MunstermanZull Ise HishamNoch keine Bewertungen
- PCBL Regulations SummaryDokument6 SeitenPCBL Regulations SummaryEugene A. EstacioNoch keine Bewertungen
- Name AddressDokument2 SeitenName Addressapi-346543590Noch keine Bewertungen
- Funda of Games SportsDokument7 SeitenFunda of Games SportsJessaNoch keine Bewertungen
- Coach Javorek's Lifelong Impact on Strength and ConditioningDokument10 SeitenCoach Javorek's Lifelong Impact on Strength and Conditioningvampyre30875% (4)
- Warm-Up Exercises For Table TennisDokument12 SeitenWarm-Up Exercises For Table TennisEmma OmictinNoch keine Bewertungen
- Nevada Sagebrush Archives 11/03/09Dokument22 SeitenNevada Sagebrush Archives 11/03/09The Nevada SagebrushNoch keine Bewertungen
- 16 - 2010 TFS 68 StickDokument31 Seiten16 - 2010 TFS 68 StickTom Hochhalter100% (1)
- Data InterpretationDokument12 SeitenData InterpretationNAGU NNoch keine Bewertungen
- A. The Relationship Between Training Load and Injury in AthletesDokument33 SeitenA. The Relationship Between Training Load and Injury in Athletespaulo tsunetaNoch keine Bewertungen
- Women's home fitness equipment purchasesDokument9 SeitenWomen's home fitness equipment purchasesRaj MalyaNoch keine Bewertungen
- From The Tube 3Dokument809 SeitenFrom The Tube 3Pcnhs SalNoch keine Bewertungen
- Brochure Sports LightingDokument40 SeitenBrochure Sports Lightingjust_4_u_dear_in9549Noch keine Bewertungen
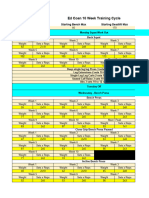
- Ed Coan 10 Week ProgrammeDokument6 SeitenEd Coan 10 Week ProgrammePjNoch keine Bewertungen
- GS Preliminary Exam Practice TestDokument21 SeitenGS Preliminary Exam Practice Test5.Đức DũngNoch keine Bewertungen
- The New Polo GT Tdi & Tsi: SpecificationsDokument2 SeitenThe New Polo GT Tdi & Tsi: SpecificationsNabajit KakatiNoch keine Bewertungen
- Hall of Fame List Per EventDokument18 SeitenHall of Fame List Per Eventapi-411258154100% (1)
- Mercyhurst Magazine - Fall 1991Dokument40 SeitenMercyhurst Magazine - Fall 1991hurstalumniNoch keine Bewertungen
- Automan June 2011Dokument83 SeitenAutoman June 2011Automan MagazineNoch keine Bewertungen
- Shaft Drive Vs Chain DriveDokument3 SeitenShaft Drive Vs Chain DriveSubroto MukerjiNoch keine Bewertungen