Das könnte Ihnen auch gefallen
- Rocker Switches Part 2Dokument28 SeitenRocker Switches Part 2Taha HashmiNoch keine Bewertungen
- Aircraft Data ComparisonDokument10 SeitenAircraft Data ComparisonTaha HashmiNoch keine Bewertungen
- A318 6 - 51-57 Diff L3 (1 CMP)Dokument30 SeitenA318 6 - 51-57 Diff L3 (1 CMP)Taha Hashmi100% (1)
- Effect of Longitudinal Stability On Different Aircraft ConfigurationsDokument14 SeitenEffect of Longitudinal Stability On Different Aircraft ConfigurationsTaha HashmiNoch keine Bewertungen
- Advanced Fuel & Ignition2Dokument11 SeitenAdvanced Fuel & Ignition2Taha HashmiNoch keine Bewertungen
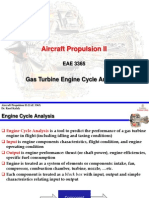
- Aircraft Propulsion II: Gas Turbine Engine Cycle AnalysisDokument61 SeitenAircraft Propulsion II: Gas Turbine Engine Cycle AnalysisTaha HashmiNoch keine Bewertungen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Distribution BoardDokument7 SeitenDistribution BoardmuralichandrasekarNoch keine Bewertungen
- Grade 9 WorkbookDokument44 SeitenGrade 9 WorkbookMaria Russeneth Joy NaloNoch keine Bewertungen
- Tachycardia Algorithm 2021Dokument1 SeiteTachycardia Algorithm 2021Ravin DebieNoch keine Bewertungen
- Lesson: The Averys Have Been Living in New York Since The Late NinetiesDokument1 SeiteLesson: The Averys Have Been Living in New York Since The Late NinetiesLinea SKDNoch keine Bewertungen
- Oracle SOA Suite 11g:buildDokument372 SeitenOracle SOA Suite 11g:buildMohsen Tavakkoli100% (1)
- Business CombinationsDokument18 SeitenBusiness Combinationszubair afzalNoch keine Bewertungen
- Daikin FUW Cabinet Fan Coil UnitDokument29 SeitenDaikin FUW Cabinet Fan Coil UnitPaul Mendoza100% (1)
- 100 20210811 ICOPH 2021 Abstract BookDokument186 Seiten100 20210811 ICOPH 2021 Abstract Bookwafiq alibabaNoch keine Bewertungen
- Engine Controls (Powertrain Management) - ALLDATA RepairDokument3 SeitenEngine Controls (Powertrain Management) - ALLDATA RepairRonald FerminNoch keine Bewertungen
- Historical Exchange Rates - OANDA AUD-MYRDokument1 SeiteHistorical Exchange Rates - OANDA AUD-MYRML MLNoch keine Bewertungen
- Session4 Automotive Front End DesignDokument76 SeitenSession4 Automotive Front End DesignShivprasad SavadattiNoch keine Bewertungen
- Japanese GardensDokument22 SeitenJapanese GardensAnmol ChughNoch keine Bewertungen
- Bluestar Annual Report 2021-22Dokument302 SeitenBluestar Annual Report 2021-22Kunal PohaniNoch keine Bewertungen
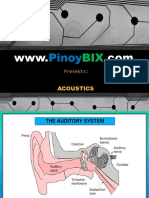
- AcousticsDokument122 SeitenAcousticsEclipse YuNoch keine Bewertungen
- Lesson Plan SustainabilityDokument5 SeitenLesson Plan Sustainabilityapi-501066857Noch keine Bewertungen
- Sistine Chapel Ceiling Lesson PlanDokument28 SeitenSistine Chapel Ceiling Lesson PlannivamNoch keine Bewertungen
- Dialog InggrisDokument4 SeitenDialog Inggrisبايو سيتياوانNoch keine Bewertungen
- Ymrtc LogDokument26 SeitenYmrtc LogVinicius Silveira0% (1)
- Progress Report 1Dokument3 SeitenProgress Report 1api-302815786Noch keine Bewertungen
- Settlement Report - 14feb17Dokument10 SeitenSettlement Report - 14feb17Abdul SalamNoch keine Bewertungen
- Holiday AssignmentDokument18 SeitenHoliday AssignmentAadhitya PranavNoch keine Bewertungen
- Christena Nippert-Eng - Watching Closely - A Guide To Ethnographic Observation-Oxford University Press (2015)Dokument293 SeitenChristena Nippert-Eng - Watching Closely - A Guide To Ethnographic Observation-Oxford University Press (2015)Emiliano CalabazaNoch keine Bewertungen
- Model TB-16Dokument20 SeitenModel TB-16xuanphuong2710Noch keine Bewertungen
- III.A.1. University of Hawaii at Manoa Cancer Center Report and Business PlanDokument35 SeitenIII.A.1. University of Hawaii at Manoa Cancer Center Report and Business Planurindo mars29Noch keine Bewertungen
- Life in The Ancient WorldDokument48 SeitenLife in The Ancient Worldjmagil6092100% (1)
- Oral ComDokument2 SeitenOral ComChristian OwlzNoch keine Bewertungen
- WinCC Control CenterDokument300 SeitenWinCC Control Centerwww.otomasyonegitimi.comNoch keine Bewertungen
- AstmDokument5 SeitenAstmyanurarzaqaNoch keine Bewertungen
- Code ExplanantionDokument4 SeitenCode ExplanantionVivek JadiyaNoch keine Bewertungen
- LavazzaDokument2 SeitenLavazzajendakimNoch keine Bewertungen