Das könnte Ihnen auch gefallen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Investigation Formats2Dokument45 SeitenInvestigation Formats2Lhine Kiwalan100% (1)
- Glossary of Important Terms For Evaluation and Assessment As A Precursor To Solicitation of GrantsDokument8 SeitenGlossary of Important Terms For Evaluation and Assessment As A Precursor To Solicitation of GrantsbobbysingersyahooNoch keine Bewertungen
- Special Laws On Children - 8353 9262 9231 7877 7610 920-130608212650Dokument95 SeitenSpecial Laws On Children - 8353 9262 9231 7877 7610 920-130608212650bobbysingersyahooNoch keine Bewertungen
- Case Report Original Article: Utilization Pa! Ern of Psychiatric Consultation ServicesDokument7 SeitenCase Report Original Article: Utilization Pa! Ern of Psychiatric Consultation ServicesbobbysingersyahooNoch keine Bewertungen
- DSWDDokument61 SeitenDSWDGorby Resuello89% (9)
- CSC Form 41 - Medical CertifcateDokument1 SeiteCSC Form 41 - Medical CertifcateRizal LeonardoNoch keine Bewertungen
- CNSP FileDokument3 SeitenCNSP FilebobbysingersyahooNoch keine Bewertungen
- 111 The Law ChicDokument14 Seiten111 The Law ChicbobbysingersyahooNoch keine Bewertungen
- Mens Rea Table - NewDokument4 SeitenMens Rea Table - NewbobbysingersyahooNoch keine Bewertungen
- Children With ProblemsDokument97 SeitenChildren With ProblemsbobbysingersyahooNoch keine Bewertungen
- Exponential EquationDokument77 SeitenExponential EquationbobbysingersyahooNoch keine Bewertungen
- Firo - B: Will SchutzDokument10 SeitenFiro - B: Will SchutzAshokNoch keine Bewertungen
- Bill of Rights - Section6-12Dokument23 SeitenBill of Rights - Section6-12sydfrey75% (4)
- JC2013-1 AnnexbDokument20 SeitenJC2013-1 AnnexbJeremiah TrinidadNoch keine Bewertungen
- Counselor S Check List of Rights and ResponsibilitiesDokument3 SeitenCounselor S Check List of Rights and ResponsibilitiesbobbysingersyahooNoch keine Bewertungen
- TODA JR vs. Court of Appeals DigestDokument2 SeitenTODA JR vs. Court of Appeals Digestproject_zi50% (2)
- What Is Night Shift Differential PayDokument14 SeitenWhat Is Night Shift Differential PaybobbysingersyahooNoch keine Bewertungen
- The Attorney General's Guidelines For Domestic Fbi OperationsDokument46 SeitenThe Attorney General's Guidelines For Domestic Fbi Operationsmary engNoch keine Bewertungen
- JC2013-1 Annex A.1Dokument1 SeiteJC2013-1 Annex A.1bobbysingersyahooNoch keine Bewertungen
- FIRODokument4 SeitenFIROsheerinfathimaNoch keine Bewertungen
- Firo-B PowrpointDokument34 SeitenFiro-B PowrpointbobbysingersyahooNoch keine Bewertungen
- Cases On Wills and SuccessionDokument4 SeitenCases On Wills and SuccessionDeb BagaporoNoch keine Bewertungen
- Children's Personality QuestionnaireDokument138 SeitenChildren's Personality QuestionnairebobbysingersyahooNoch keine Bewertungen
- FIRODokument1 SeiteFIROTamanna SarkarNoch keine Bewertungen
- Mens Rea Table PDFDokument2 SeitenMens Rea Table PDFbobbysingersyahooNoch keine Bewertungen
- AphasiaDokument2 SeitenAphasiaVanessa AntoineNoch keine Bewertungen
- Psychometric Tests For Recuitment and Selection ProjectDokument75 SeitenPsychometric Tests For Recuitment and Selection Projectbobbysingersyahoo100% (1)
- Important Decisions Thirty Year Cut OffDokument45 SeitenImportant Decisions Thirty Year Cut OffbobbysingersyahooNoch keine Bewertungen
- Feb 28proceedings Notes FinalDokument102 SeitenFeb 28proceedings Notes FinalbobbysingersyahooNoch keine Bewertungen
- Lions Digests IIDokument16 SeitenLions Digests IIbobbysingersyahooNoch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Chem Sba 2019-2020Dokument36 SeitenChem Sba 2019-2020Amma MissigherNoch keine Bewertungen
- Web Script Ems Core 4 Hernandez - Gene Roy - 07!22!2020Dokument30 SeitenWeb Script Ems Core 4 Hernandez - Gene Roy - 07!22!2020gene roy hernandezNoch keine Bewertungen
- Topic: Going To and Coming From Place of WorkDokument2 SeitenTopic: Going To and Coming From Place of WorkSherry Jane GaspayNoch keine Bewertungen
- Interventional Cardiology and SurgeryDokument19 SeitenInterventional Cardiology and SurgeryDEV NANDHINI RNoch keine Bewertungen
- UNICEF Annual Report - Water 2018Dokument20 SeitenUNICEF Annual Report - Water 2018Ross WeistrofferNoch keine Bewertungen
- Amniotic Fluid DisordersDokument16 SeitenAmniotic Fluid DisordersLytiana Williams100% (2)
- Monitor Zoncare - PM-8000 ServicemanualDokument83 SeitenMonitor Zoncare - PM-8000 Servicemanualwilmer100% (1)
- Cardiovascular SystemDokument47 SeitenCardiovascular SystemAtnasiya GadisaNoch keine Bewertungen
- Service Manual - DM0412SDokument11 SeitenService Manual - DM0412SStefan Jovanovic100% (1)
- Screenshot 2019-10-30 at 12.44.00Dokument25 SeitenScreenshot 2019-10-30 at 12.44.00Miền VũNoch keine Bewertungen
- Research Paper DraftDokument45 SeitenResearch Paper DraftMelissa SpamNoch keine Bewertungen
- Review Factors Contributing To Medication Errors: A Literature ReviewDokument9 SeitenReview Factors Contributing To Medication Errors: A Literature Reviewsoul_0602Noch keine Bewertungen
- Mapagbigay PT1 Group1Dokument4 SeitenMapagbigay PT1 Group1Hazel SarmientoNoch keine Bewertungen
- Wax Depilation ManualDokument17 SeitenWax Depilation ManualAmit Sharma100% (1)
- GEC PE 3 ModuleDokument72 SeitenGEC PE 3 ModuleMercy Anne EcatNoch keine Bewertungen
- Uji Stabilitas Tablet Floating Ranitidin HCL: Pengaruhnya Terhadap Sifat Fisik Dan Profil Disolusi Dalam Medium SGF Tanpa PepsinDokument16 SeitenUji Stabilitas Tablet Floating Ranitidin HCL: Pengaruhnya Terhadap Sifat Fisik Dan Profil Disolusi Dalam Medium SGF Tanpa PepsinZeaa MaysNoch keine Bewertungen
- EMC Design GuideDokument42 SeitenEMC Design GuideDe Raghu Veer KNoch keine Bewertungen
- Muet Topic 10 City Life Suggested Answer and IdiomsDokument3 SeitenMuet Topic 10 City Life Suggested Answer and IdiomsMUHAMAD FAHMI BIN SHAMSUDDIN MoeNoch keine Bewertungen
- Datasheet Cofraplus 60Dokument2 SeitenDatasheet Cofraplus 60Žarko JanjićNoch keine Bewertungen
- Air Conditioning Is Inoperative, Fault Code 91eb11 or 91eb15 Is StoredDokument5 SeitenAir Conditioning Is Inoperative, Fault Code 91eb11 or 91eb15 Is Storedwasim AiniaNoch keine Bewertungen
- CW Catalogue Cables and Wires A4 En-2Dokument1.156 SeitenCW Catalogue Cables and Wires A4 En-2Ovidiu PuieNoch keine Bewertungen
- WWW - Devicemanuals.eu: GardenaDokument6 SeitenWWW - Devicemanuals.eu: GardenapotoculNoch keine Bewertungen
- Nfpa Training - Nfpa 72Dokument107 SeitenNfpa Training - Nfpa 72yusuf.ahmediutNoch keine Bewertungen
- Book Report British Airways Flight 5390Dokument7 SeitenBook Report British Airways Flight 5390KaruNoch keine Bewertungen
- The Man Booker PrizeDokument2 SeitenThe Man Booker PrizeChu Hòa Bình100% (1)
- Molecular MechanicsDokument26 SeitenMolecular MechanicsKarthi ShanmugamNoch keine Bewertungen
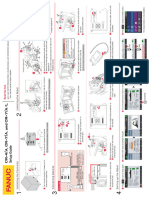
- CR-7iA CR-4iA Installation and Setup Guide (B-83774JA-1 01)Dokument1 SeiteCR-7iA CR-4iA Installation and Setup Guide (B-83774JA-1 01)lidiia.pavlkukNoch keine Bewertungen
- Reading Test - 3 Clinical Depression Text ADokument17 SeitenReading Test - 3 Clinical Depression Text AJisha JanardhanNoch keine Bewertungen
- Figs Taste Scale of Selected Varieties From Hawaiifruit-Net PDFDokument4 SeitenFigs Taste Scale of Selected Varieties From Hawaiifruit-Net PDFHanafizar Hanafi Napi AtanNoch keine Bewertungen
- Ronnel Del RioDokument5 SeitenRonnel Del Rioamity balweg100% (2)