Das könnte Ihnen auch gefallen
- Problem-based Approach to Gastroenterology and HepatologyVon EverandProblem-based Approach to Gastroenterology and HepatologyJohn N. PlevrisNoch keine Bewertungen
- 418 Lilo Nidoira Case Scenario.Dokument7 Seiten418 Lilo Nidoira Case Scenario.Raymart SubejanoNoch keine Bewertungen
- Core Competencies in Nursing-1Dokument11 SeitenCore Competencies in Nursing-1yakapmNoch keine Bewertungen
- Hirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsVon EverandHirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNoch keine Bewertungen
- BSN3-1 Perioperative-Nursing 2021Dokument236 SeitenBSN3-1 Perioperative-Nursing 2021Ms MedSurg Nursin100% (2)
- ICU Scoring Systems A Complete Guide - 2020 EditionVon EverandICU Scoring Systems A Complete Guide - 2020 EditionNoch keine Bewertungen
- Tracheostomy DR KVLN Rao PDFDokument33 SeitenTracheostomy DR KVLN Rao PDFVenkata Krishna Kanth ThippanaNoch keine Bewertungen
- HCVDDokument99 SeitenHCVDMiguel CuevasNoch keine Bewertungen
- Trauma and Emergency NursingDokument9 SeitenTrauma and Emergency Nursingchinthaka18389021Noch keine Bewertungen
- Operation Theater 1Dokument24 SeitenOperation Theater 1Susmita BeheraNoch keine Bewertungen
- Endoscopicretrograde Cholangiopancreatography (ERCP)Dokument21 SeitenEndoscopicretrograde Cholangiopancreatography (ERCP)Suman PokhrelNoch keine Bewertungen
- Position of PatientDokument47 SeitenPosition of PatientMuhammad Al-azzizNoch keine Bewertungen
- Chapter 7 The Nurse-Client Relationship PDFDokument9 SeitenChapter 7 The Nurse-Client Relationship PDFJa YaNoch keine Bewertungen
- Early Warning Score For Patient Safety Measures - Mohd Said NurumalDokument50 SeitenEarly Warning Score For Patient Safety Measures - Mohd Said NurumalAiko himeNoch keine Bewertungen
- Penetrating Abdominal TraumaDokument67 SeitenPenetrating Abdominal TraumarizkaNoch keine Bewertungen
- 8-Wounds and Wound Healing-1Dokument31 Seiten8-Wounds and Wound Healing-1Aiden JosephatNoch keine Bewertungen
- Triage and Disaster: Nur Masyeerah Abdul JalilDokument22 SeitenTriage and Disaster: Nur Masyeerah Abdul JalilnavenNoch keine Bewertungen
- Top 10 Care Essentials in Ventilated PtsDokument3 SeitenTop 10 Care Essentials in Ventilated PtsAdel HamadaNoch keine Bewertungen
- Tracheostomy Tubesuctioning2 MikeDokument29 SeitenTracheostomy Tubesuctioning2 MikeClaudia VillalunaNoch keine Bewertungen
- Thrombolytics (Fibrinolytics)Dokument14 SeitenThrombolytics (Fibrinolytics)J lodhiNoch keine Bewertungen
- ABCs of Thoracic TraumaDokument5 SeitenABCs of Thoracic TraumaAlice S ChangNoch keine Bewertungen
- Initial Assessment and ManagementDokument8 SeitenInitial Assessment and ManagementAlvin De LunaNoch keine Bewertungen
- Case Presentation Laryngitis TB 70 TahunDokument21 SeitenCase Presentation Laryngitis TB 70 TahunMegan Shanzu100% (1)
- COMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideVon EverandCOMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideNoch keine Bewertungen
- Ebstein Anomaly, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsVon EverandEbstein Anomaly, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNoch keine Bewertungen
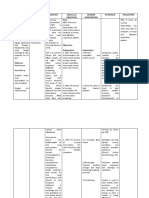
- Cues Nursing Diagnosis Analysis GOALS and Objectives Nursing Intervention Rationale Evaluation Subjective: GoalDokument4 SeitenCues Nursing Diagnosis Analysis GOALS and Objectives Nursing Intervention Rationale Evaluation Subjective: GoalMonica Angelique SalayoNoch keine Bewertungen
- Acute Biologic CrisisDokument142 SeitenAcute Biologic CrisisAngel VallejoNoch keine Bewertungen
- Severe Asthma ChildrenDokument4 SeitenSevere Asthma ChildreneddcitoNoch keine Bewertungen
- Enabling Learning in Nursing and Midwifery Practice: A Guide for MentorsVon EverandEnabling Learning in Nursing and Midwifery Practice: A Guide for MentorsSue WestNoch keine Bewertungen
- Hemodynamic MonitoringDokument4 SeitenHemodynamic Monitoringgurneet kourNoch keine Bewertungen
- Skin Integrity and Wound CareDokument47 SeitenSkin Integrity and Wound CareCHALIE MEQUNoch keine Bewertungen
- Management of Arterial LineDokument16 SeitenManagement of Arterial LineFarcasanu Liana GeorgianaNoch keine Bewertungen
- TracheotomyDokument19 SeitenTracheotomyKarina BundaNoch keine Bewertungen
- Documentation and Reporting SlideDokument30 SeitenDocumentation and Reporting SlideChristille Grace Basa MuchuelasNoch keine Bewertungen
- Genitourinary Assessment: Jan Bazner-Chandler RN, MSN, CNS, CPNPDokument27 SeitenGenitourinary Assessment: Jan Bazner-Chandler RN, MSN, CNS, CPNPJason Nisky100% (1)
- Perioperatif Nursing PDFDokument93 SeitenPerioperatif Nursing PDFNurvanny HusnaNoch keine Bewertungen
- Devices Used in ICU: Critical Care NursingDokument95 SeitenDevices Used in ICU: Critical Care NursinghendranatjNoch keine Bewertungen
- Introduction To Patient SafetyDokument54 SeitenIntroduction To Patient Safetyrejoicedear2020Noch keine Bewertungen
- HYDROCEPHALUSDokument63 SeitenHYDROCEPHALUSAjeng Aristiany Rahawarin100% (2)
- Checklist For Cardiac AssessmentDokument3 SeitenChecklist For Cardiac AssessmentCake ManNoch keine Bewertungen
- Hepatic Encephalopathy and ComaDokument19 SeitenHepatic Encephalopathy and ComaJas Castro JoveroNoch keine Bewertungen
- Nursing Assessment Tool... CardiacDokument7 SeitenNursing Assessment Tool... Cardiacjai2xNoch keine Bewertungen
- URINALYSISDokument3 SeitenURINALYSISmimaiax100% (4)
- CPR Checklist PDFDokument2 SeitenCPR Checklist PDFSakura SaitoNoch keine Bewertungen
- Icu Equipments BY: Presented Bhupender Kumar MehtoDokument35 SeitenIcu Equipments BY: Presented Bhupender Kumar Mehtobhupendermehto012Noch keine Bewertungen
- Pathology Intro Part 1 PDFDokument13 SeitenPathology Intro Part 1 PDFAmy LalringhluaniNoch keine Bewertungen
- GI Diagnostic TestsDokument7 SeitenGI Diagnostic TestspatzieNoch keine Bewertungen
- Cardiorespiratory Arrest (FS)Dokument88 SeitenCardiorespiratory Arrest (FS)haerul ikhsanNoch keine Bewertungen
- Early Warning Score & Rapid Response TeamDokument26 SeitenEarly Warning Score & Rapid Response TeamAsim IdreesNoch keine Bewertungen
- Muscle Strength TestingDokument3 SeitenMuscle Strength TestingGiselle Chloe Baluya ico100% (1)
- Cardiac TestsDokument17 SeitenCardiac TestsGiorgiana pNoch keine Bewertungen
- FR Dur I Ski'ta - S: SK Ti 25-f $kifiDokument6 SeitenFR Dur I Ski'ta - S: SK Ti 25-f $kifijerayne50% (2)
- Group 5 - Hemodialysis - Chronic Kidney FailureDokument31 SeitenGroup 5 - Hemodialysis - Chronic Kidney FailureKimberly Abella CabreraNoch keine Bewertungen
- Week 4 Ethics Decision MakingDokument59 SeitenWeek 4 Ethics Decision Makingmaha abdallahNoch keine Bewertungen
- 13.knowledge and Practices of Universal Precautions Among Basic B. Sc. Nursing StudentsDokument10 Seiten13.knowledge and Practices of Universal Precautions Among Basic B. Sc. Nursing StudentsPutri Alin Kende RiaralyNoch keine Bewertungen
- Primary Trauma CareDokument48 SeitenPrimary Trauma CareKABERA RENENoch keine Bewertungen
- Atlas of Trauma: Operative Techniques, Complications and ManagementVon EverandAtlas of Trauma: Operative Techniques, Complications and ManagementPaula FerradaNoch keine Bewertungen
- ThrombophlebitisDokument3 SeitenThrombophlebitismirrejNoch keine Bewertungen
- Initial Assessment & ManagementDokument3 SeitenInitial Assessment & Managementjc_sibal13Noch keine Bewertungen
- TraumaDokument2 SeitenTraumajc_sibal13Noch keine Bewertungen
- Basic Life SupportDokument3 SeitenBasic Life Supportjc_sibal13Noch keine Bewertungen
- Surgical MetabolismDokument10 SeitenSurgical Metabolismjc_sibal13Noch keine Bewertungen
- Pediatric and Elderly Patients in SurgeryDokument4 SeitenPediatric and Elderly Patients in Surgeryjc_sibal13Noch keine Bewertungen
- Surgical InfectionsDokument2 SeitenSurgical Infectionsjc_sibal13100% (1)
- Surgical Infections Surgical Infections: HistoryDokument7 SeitenSurgical Infections Surgical Infections: Historyjc_sibal13Noch keine Bewertungen
- Fluids and ElectrolytesDokument10 SeitenFluids and Electrolytesjc_sibal13Noch keine Bewertungen
- Surgical MetabolismDokument12 SeitenSurgical Metabolismjc_sibal13Noch keine Bewertungen
- Fluids and ElectrolytesDokument16 SeitenFluids and Electrolytesjc_sibal13Noch keine Bewertungen
- Systemic Response To InjuryDokument7 SeitenSystemic Response To Injuryjc_sibal13Noch keine Bewertungen
- ShockDokument3 SeitenShockjc_sibal13Noch keine Bewertungen
- Metabolism in SurgeryDokument5 SeitenMetabolism in Surgeryjc_sibal13Noch keine Bewertungen
- Systemic Response To InjuryDokument2 SeitenSystemic Response To Injuryjc_sibal13100% (1)
- Bleeding and Transfusion: Section I ResuscitationDokument22 SeitenBleeding and Transfusion: Section I Resuscitationjc_sibal13Noch keine Bewertungen
- Discuss The Essentials of Hemostasis and Surgical BleedingDokument17 SeitenDiscuss The Essentials of Hemostasis and Surgical Bleedingjc_sibal13Noch keine Bewertungen
- Discuss The Essentials of Hemostasis and Surgical BleedingDokument5 SeitenDiscuss The Essentials of Hemostasis and Surgical Bleedingjc_sibal13Noch keine Bewertungen
- Discuss The Essentials of Hemostasis and Surgical BleedingDokument10 SeitenDiscuss The Essentials of Hemostasis and Surgical Bleedingjc_sibal13Noch keine Bewertungen
- Wound Healing Wound Healing and Wound and Wound Care Care Care CareDokument7 SeitenWound Healing Wound Healing and Wound and Wound Care Care Care Carejc_sibal13Noch keine Bewertungen
- EXAM QUESTIONS On Wound Healing and Surgical Site InfectionsDokument2 SeitenEXAM QUESTIONS On Wound Healing and Surgical Site Infectionsjc_sibal13Noch keine Bewertungen
- Wound Care and Wound Healing - Dr. Alex A. ErasmoDokument1 SeiteWound Care and Wound Healing - Dr. Alex A. Erasmojc_sibal13Noch keine Bewertungen
- Clinical Outcome Assessments in Duchenne Muscular Dystrophy - 2021 - NeuromusculDokument10 SeitenClinical Outcome Assessments in Duchenne Muscular Dystrophy - 2021 - NeuromusculSuzie Simone Mardones SilvaNoch keine Bewertungen
- Pearls of MRCP Part 2 PastestDokument111 SeitenPearls of MRCP Part 2 PastestS TNoch keine Bewertungen
- Bmi ProjectDokument44 SeitenBmi ProjectPrince Bhaskar100% (1)
- A Mini-Review For Causes, Effects and Preventive Measures of Choking SmogDokument6 SeitenA Mini-Review For Causes, Effects and Preventive Measures of Choking SmogChoudhry TradersNoch keine Bewertungen
- Introduction To ImunologiDokument32 SeitenIntroduction To ImunologiNur AisyahhNoch keine Bewertungen
- TVL - Module 11 Perform Manicure and Pedicure Real Na TalagaDokument64 SeitenTVL - Module 11 Perform Manicure and Pedicure Real Na Talagaberna mcmenNoch keine Bewertungen
- Headache: Migraine and Tension-Type HeadacheDokument12 SeitenHeadache: Migraine and Tension-Type HeadacheLoren SangalangNoch keine Bewertungen
- 1700 Questions Not in PLABABLEDokument131 Seiten1700 Questions Not in PLABABLEDaniah Marwan Dawood DAWOODNoch keine Bewertungen
- Document 32Dokument3 SeitenDocument 32Grace CruzNoch keine Bewertungen
- ( ( ( (The Luo Vessels) ) ) ) : Paula Chin's Class Notes Fall 2003Dokument66 Seiten( ( ( (The Luo Vessels) ) ) ) : Paula Chin's Class Notes Fall 2003DK100% (1)
- Ear Pain Flow Chart: Homeopathic Remedy GuideDokument4 SeitenEar Pain Flow Chart: Homeopathic Remedy GuideAtit Sheth100% (1)
- Tuto Respiratory SystemDokument3 SeitenTuto Respiratory SystemIlya ZafirahNoch keine Bewertungen
- Neurological DisordersDokument10 SeitenNeurological DisorderssoumenNoch keine Bewertungen
- Gangguan Hemodinamik, Trombosis Dan Syok: Fk-Uncen JayapuraDokument67 SeitenGangguan Hemodinamik, Trombosis Dan Syok: Fk-Uncen Jayapuramarsal25Noch keine Bewertungen
- F. Physical Assessment: 5. EyesDokument47 SeitenF. Physical Assessment: 5. EyesJuliane100% (1)
- Dept ENT PDFDokument117 SeitenDept ENT PDFPravee GaddeNoch keine Bewertungen
- Cardiopulmonary Resuscitation: Unit 7Dokument15 SeitenCardiopulmonary Resuscitation: Unit 7حيدر الاسديNoch keine Bewertungen
- Marieb Human Anatomy Physiology 12Th Edition Katja Hoehn Full ChapterDokument67 SeitenMarieb Human Anatomy Physiology 12Th Edition Katja Hoehn Full Chapterzoe.boulton781100% (6)
- 107 NLE Leadership and Management QuestionDokument4 Seiten107 NLE Leadership and Management QuestionMae Montesena Breganza100% (1)
- Abordaje de Paciente Con SoploDokument11 SeitenAbordaje de Paciente Con SoploRigo rogerNoch keine Bewertungen
- Sample Pandemic Continuity PlanDokument17 SeitenSample Pandemic Continuity Planiulian1977Noch keine Bewertungen
- Function and Disorder of Adrenal GlandDokument2 SeitenFunction and Disorder of Adrenal GlandSuneel Kumar PrajapatiNoch keine Bewertungen
- Health History and Physical Assessment On Patient With COPDDokument4 SeitenHealth History and Physical Assessment On Patient With COPDDjameica GuerreroNoch keine Bewertungen
- A26 - Walk in Paschim Vihar Ii: NoteDokument2 SeitenA26 - Walk in Paschim Vihar Ii: NoteLakshay MahajanNoch keine Bewertungen
- Cartones Bingo 75 BolasDokument10 SeitenCartones Bingo 75 BolasJAVI GUENoch keine Bewertungen
- BRS PediatricsDokument971 SeitenBRS Pediatricstycobb6371% (7)
- Pharmacotherapeutics For Nurse Pract. Prescribers 2nd Ed. - A. Wynne, Et. Al., (F. A. Davis, 2007) WWDokument1.351 SeitenPharmacotherapeutics For Nurse Pract. Prescribers 2nd Ed. - A. Wynne, Et. Al., (F. A. Davis, 2007) WWcatalin calinNoch keine Bewertungen
- Hernia: Inguinal - Surgical Anatomy, Presentation, Treatment, ComplicationsDokument37 SeitenHernia: Inguinal - Surgical Anatomy, Presentation, Treatment, ComplicationsIvan Olo SarumpaetNoch keine Bewertungen
- Career Opportunities in Medical TechnologyDokument10 SeitenCareer Opportunities in Medical TechnologyMariah Kristine AprodaNoch keine Bewertungen
- What Is DepressionDokument2 SeitenWhat Is DepressionFeb NamiaNoch keine Bewertungen