Das könnte Ihnen auch gefallen
- Sample PPE Request FormDokument2 SeitenSample PPE Request FormMaurice Balkissoon60% (15)
- Return of The Runelords - Player's Guide PDFDokument14 SeitenReturn of The Runelords - Player's Guide PDFPablo Herrer100% (5)
- A91 C Workshop ManualDokument318 SeitenA91 C Workshop ManualDylan Mitchell100% (1)
- Iyengar Yoga Home Practice Sequences 1 PDFDokument4 SeitenIyengar Yoga Home Practice Sequences 1 PDFYogesh Sharma100% (1)
- Myofascial Release TechniqueDokument72 SeitenMyofascial Release TechniqueAnuj Agarwal75% (4)
- Restore Scapula Control for Thoracic Outlet SyndromeDokument10 SeitenRestore Scapula Control for Thoracic Outlet Syndromercastello20Noch keine Bewertungen
- A4 - in The Dungeons of The Slave LordsDokument36 SeitenA4 - in The Dungeons of The Slave LordsSturm75% (4)
- Hydraulic Seal Identification ChartDokument29 SeitenHydraulic Seal Identification ChartAnonymous K6mLK72AaNoch keine Bewertungen
- Manual Therapy Lecture 4Dokument33 SeitenManual Therapy Lecture 4abrarhsyn2020Noch keine Bewertungen
- Fascia and Fascia Lines PDFDokument7 SeitenFascia and Fascia Lines PDFBeta LisboaNoch keine Bewertungen
- 32 Understanding Fibroblasts in Order To Comprehend The Osteopathic Treatment of The FasciaDokument8 Seiten32 Understanding Fibroblasts in Order To Comprehend The Osteopathic Treatment of The FasciaRenan O. Pravatta PivettaNoch keine Bewertungen
- BetterOrthopedics 2nd-EdLesondak ChapterDokument12 SeitenBetterOrthopedics 2nd-EdLesondak Chapter施凯Noch keine Bewertungen
- Deep fascia detailsDokument5 SeitenDeep fascia detailsMM NabeelNoch keine Bewertungen
- Advanced Anatomy - Myofascial MeridiansDokument37 SeitenAdvanced Anatomy - Myofascial MeridiansBioTaoQi100% (2)
- Journalclubsummary Tom2015jan PDFDokument3 SeitenJournalclubsummary Tom2015jan PDFCalenda JanNoch keine Bewertungen
- Pyogenic Discitis Power PointDokument121 SeitenPyogenic Discitis Power Pointjav_luv37Noch keine Bewertungen
- Muscle Physiology & Its Significance-TextDokument16 SeitenMuscle Physiology & Its Significance-TextCidVijayanNoch keine Bewertungen
- Tendon Structure and Healing ProcessDokument9 SeitenTendon Structure and Healing ProcessLuki ErtandriNoch keine Bewertungen
- FasciaDokument6 SeitenFasciakabshielNoch keine Bewertungen
- Fitness in The Extended Fascial ParadigmDokument37 SeitenFitness in The Extended Fascial Paradigmgavinbroomes100% (1)
- The Human Fascial System by L Stecco J A Day HandoutsDokument4 SeitenThe Human Fascial System by L Stecco J A Day Handoutsnyaniso rahotepNoch keine Bewertungen
- Myofascial Pain SyndromeDokument61 SeitenMyofascial Pain Syndromeyosra adam100% (1)
- BM of Softtissue AftrmsDokument52 SeitenBM of Softtissue AftrmsborrellanoNoch keine Bewertungen
- Macro Fascial MobilisationDokument15 SeitenMacro Fascial Mobilisationajimshaw100% (1)
- Muscular SystemDokument8 SeitenMuscular Systemtheodore_estradaNoch keine Bewertungen
- Muscle Physiology & Its SignificanceDokument25 SeitenMuscle Physiology & Its SignificanceTarun Goyal100% (2)
- Presentation Fascial ManipulationDokument8 SeitenPresentation Fascial ManipulationricardoNoch keine Bewertungen
- Myofascial Release ManualDokument30 SeitenMyofascial Release Manualfrancesco100% (2)
- Locomotor SlingsDokument4 SeitenLocomotor SlingsPhooi Yee LauNoch keine Bewertungen
- Laprak MuscleDokument12 SeitenLaprak MuscleRezky AmaliahNoch keine Bewertungen
- Bio Dynamics The Fascia of The Pelvic Floor Model of TensegrityDokument8 SeitenBio Dynamics The Fascia of The Pelvic Floor Model of TensegritygabrielsantosmsNoch keine Bewertungen
- Fascial Fitness Training in The Neuromyofascial Web1 PDFDokument11 SeitenFascial Fitness Training in The Neuromyofascial Web1 PDFRoginicD100% (1)
- Understanding FasciaDokument7 SeitenUnderstanding FasciaWhisperer BowenNoch keine Bewertungen
- Skeletal Muscle - WikipediaDokument42 SeitenSkeletal Muscle - Wikipediacomedy videoNoch keine Bewertungen
- Fascia in Myofascial PainDokument11 SeitenFascia in Myofascial PainJulia RechulaNoch keine Bewertungen
- Riggs Grant PDFDokument18 SeitenRiggs Grant PDFcelliasttNoch keine Bewertungen
- Human Anatomy and Physiology W3 - EmmanuelaDokument5 SeitenHuman Anatomy and Physiology W3 - EmmanuelaRamizNoch keine Bewertungen
- Pathophysiology of Ligament Injuries-1Dokument21 SeitenPathophysiology of Ligament Injuries-1abdul haseebNoch keine Bewertungen
- TMJ AnatomyDokument68 SeitenTMJ AnatomyArchanaShenoyNoch keine Bewertungen
- Commentary The Indeterminable Resilience of The Fascial SystemDokument7 SeitenCommentary The Indeterminable Resilience of The Fascial SystemmarcelonorisNoch keine Bewertungen
- Chronic Osteomyelitis Case StudyDokument35 SeitenChronic Osteomyelitis Case StudyMelissa Gines100% (2)
- DefinitionDokument9 SeitenDefinitionaimiorreNoch keine Bewertungen
- Lecture Notes On The Muscular SystemDokument46 SeitenLecture Notes On The Muscular SystemDennis Nabor Muñoz, RN,RM100% (1)
- Soft Tissue DysfunctionDokument8 SeitenSoft Tissue DysfunctionphysioaliNoch keine Bewertungen
- Title: Structure & Function of Living CellsDokument10 SeitenTitle: Structure & Function of Living CellsFatima Al SayyedNoch keine Bewertungen
- 11J - Caybot - Jash Jovian - Task10Dokument11 Seiten11J - Caybot - Jash Jovian - Task10JASH JOVIAN CAYBOTNoch keine Bewertungen
- Jurnal Integumen 4Dokument12 SeitenJurnal Integumen 4Ummu AthiyyahNoch keine Bewertungen
- BiologyDokument14 SeitenBiologyNur Maisarah AnuarNoch keine Bewertungen
- Muscular TissueDokument8 SeitenMuscular TissueKaleem KhanNoch keine Bewertungen
- AnaPhysio MSDokument5 SeitenAnaPhysio MSJay Rodren IbitaNoch keine Bewertungen
- Fasciae Protectors of your Vital OrgansDokument8 SeitenFasciae Protectors of your Vital Organstito zambranoNoch keine Bewertungen
- Skeletal MuscleDokument32 SeitenSkeletal MuscleArfiNoch keine Bewertungen
- Soft Tissue Mechanics: Types and PropertiesDokument14 SeitenSoft Tissue Mechanics: Types and PropertiesKripa NNoch keine Bewertungen
- Fascial Training For More Flexibility, Suppleness and Vitality: This Is How You Get Your Fascias Into Top Form! (10 Minutes Fascia Workout For Home)Von EverandFascial Training For More Flexibility, Suppleness and Vitality: This Is How You Get Your Fascias Into Top Form! (10 Minutes Fascia Workout For Home)Noch keine Bewertungen
- Tom Myers 10 Tips For Fascial FitnessDokument11 SeitenTom Myers 10 Tips For Fascial Fitnessspiraldao100% (6)
- Zoology Notes: 011 Chapter 7Dokument4 SeitenZoology Notes: 011 Chapter 7humanupgradeNoch keine Bewertungen
- Myofascial Release: Range of Motion and FlexibilityDokument21 SeitenMyofascial Release: Range of Motion and FlexibilityMonika100% (1)
- 3.3 Muscle System As ScaffoldDokument7 Seiten3.3 Muscle System As ScaffoldSantosh hiremathNoch keine Bewertungen
- DR Bachrach Explains Prolo, ThoroughlyDokument14 SeitenDR Bachrach Explains Prolo, Thoroughlycindy.laverty5406Noch keine Bewertungen
- Pathophysio of OsteomyelitisDokument6 SeitenPathophysio of OsteomyelitisNapPeliyoNoch keine Bewertungen
- Stretching Guide for Improved MobilityDokument47 SeitenStretching Guide for Improved Mobilityphysical therapy channel ptNoch keine Bewertungen
- Biomechanics of MusclesDokument58 SeitenBiomechanics of MusclesAsad Chaudhary100% (2)
- The Tissue Level of Organization General ObjectivesDokument5 SeitenThe Tissue Level of Organization General ObjectivesRjosheNoch keine Bewertungen
- 07 Myofascial Release Techniques (1)Dokument6 Seiten07 Myofascial Release Techniques (1)Saira53 Saira53Noch keine Bewertungen
- MS 316 Lec Merge YarnDokument73 SeitenMS 316 Lec Merge YarnMARIA STEPHANY DELA CRUZNoch keine Bewertungen
- Biomechanics of Muscle (Skeletal)Dokument19 SeitenBiomechanics of Muscle (Skeletal)Murad KurdiNoch keine Bewertungen
- Fascial Training For More Flexibility, Suppleness and Vitality: This Is How You Get Your Fascias Into Top Form!Von EverandFascial Training For More Flexibility, Suppleness and Vitality: This Is How You Get Your Fascias Into Top Form!Noch keine Bewertungen
- Chapter 05Dokument15 SeitenChapter 05rcastello20Noch keine Bewertungen
- Chapter 04Dokument25 SeitenChapter 04rcastello20Noch keine Bewertungen
- Sacro Occipital Techniques Category Two A Remedy For Fixated Thinking 1352662451Dokument7 SeitenSacro Occipital Techniques Category Two A Remedy For Fixated Thinking 1352662451rcastello20Noch keine Bewertungen
- Danto AAO Convocation2012LectureDokument48 SeitenDanto AAO Convocation2012Lecturercastello20Noch keine Bewertungen
- Chapmans Reflex 1750-4732-1-10Dokument19 SeitenChapmans Reflex 1750-4732-1-10Huram-abiNoch keine Bewertungen
- 3 Drills For Improving Your Neck StrengthDokument10 Seiten3 Drills For Improving Your Neck StrengthbajetownrepNoch keine Bewertungen
- Hope - A Stroke Recovery GuideDokument20 SeitenHope - A Stroke Recovery GuideGeorgiana CotarceaNoch keine Bewertungen
- 583 FullDokument14 Seiten583 Fullrcastello20Noch keine Bewertungen
- Review Article: Force Transmission Between Synergistic Skeletal Muscles Through Connective Tissue LinkagesDokument9 SeitenReview Article: Force Transmission Between Synergistic Skeletal Muscles Through Connective Tissue Linkagesrcastello20Noch keine Bewertungen
- Three-Dimensional Mathematical Model For Deformation of Human Fasciae in Manual TherapyDokument12 SeitenThree-Dimensional Mathematical Model For Deformation of Human Fasciae in Manual Therapyrcastello20Noch keine Bewertungen
- BIOMEDICAL RESEARCH CELL BIOLOGY MEETS ROLFINGDokument2 SeitenBIOMEDICAL RESEARCH CELL BIOLOGY MEETS ROLFINGrcastello20Noch keine Bewertungen
- Strengthening Fascial Lines in 3D Using Multi-Directional TrainingDokument8 SeitenStrengthening Fascial Lines in 3D Using Multi-Directional Trainingrcastello20Noch keine Bewertungen
- 1974 OctDokument4 Seiten1974 Octrcastello20Noch keine Bewertungen
- Review Article: Force Transmission Between Synergistic Skeletal Muscles Through Connective Tissue LinkagesDokument9 SeitenReview Article: Force Transmission Between Synergistic Skeletal Muscles Through Connective Tissue Linkagesrcastello20Noch keine Bewertungen
- Cellular Biotensegrity PDFDokument15 SeitenCellular Biotensegrity PDFT4urus-VegaNoch keine Bewertungen
- Master of Physiotherapy core subjectsDokument7 SeitenMaster of Physiotherapy core subjectsrcastello20Noch keine Bewertungen
- VictoriaUniversity16022013 PDFDokument9 SeitenVictoriaUniversity16022013 PDFrcastello20Noch keine Bewertungen
- 3 Drills For Improving Your Neck StrengthDokument10 Seiten3 Drills For Improving Your Neck StrengthbajetownrepNoch keine Bewertungen
- Carta 12000 YDokument9 SeitenCarta 12000 Yrcastello20Noch keine Bewertungen
- How To Make Gravity in Scratch 3Dokument3 SeitenHow To Make Gravity in Scratch 3sonia makloufNoch keine Bewertungen
- HomeostasisDokument8 SeitenHomeostasisLely SharmaNoch keine Bewertungen
- Self-Learning Module For Grade 11Dokument14 SeitenSelf-Learning Module For Grade 11Joy S. Calayo100% (1)
- HondaDokument2 SeitenHondaMohamed Hedi RebaiNoch keine Bewertungen
- Philippine Folk Dance StepsDokument10 SeitenPhilippine Folk Dance StepsKersey BadocdocNoch keine Bewertungen
- Sportaccord, "Sport Betting and Corruption"Dokument94 SeitenSportaccord, "Sport Betting and Corruption"Tifoso BilanciatoNoch keine Bewertungen
- Serie ADokument4 SeitenSerie AJhon Hernandez RamirezNoch keine Bewertungen
- 2 Series Brochure - 0 PDFDokument4 Seiten2 Series Brochure - 0 PDFRod JesusislordNoch keine Bewertungen
- A1 - A2 - Calling Customer ServiceDokument8 SeitenA1 - A2 - Calling Customer ServiceAnderson MoraesNoch keine Bewertungen
- Granada (Free Tabs)Dokument9 SeitenGranada (Free Tabs)Rahmayuni ElsyaNoch keine Bewertungen
- The Runaway PancakeDokument15 SeitenThe Runaway PancakeSean ChangNoch keine Bewertungen
- Chess and Hip Hop QuotesDokument183 SeitenChess and Hip Hop Quotesadigtu100% (1)
- Motorsports Market Into A $5 Billion Market by 2019-IndustryARCDokument27 SeitenMotorsports Market Into A $5 Billion Market by 2019-IndustryARCAutomotiveIARCNoch keine Bewertungen
- TSR 2137 Lankhmar City of Adventure 2nd Ed - CompressDokument200 SeitenTSR 2137 Lankhmar City of Adventure 2nd Ed - CompressAstronomer855Noch keine Bewertungen
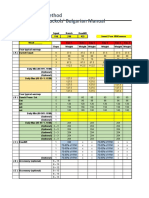
- Bulgarian Method 1Dokument9 SeitenBulgarian Method 1TRASH SHUBHAMNoch keine Bewertungen
- Challenger: MT265B / MT275B Compact TractorDokument41 SeitenChallenger: MT265B / MT275B Compact TractorMichael&Heidi ThompsonNoch keine Bewertungen
- SL 763733Dokument8 SeitenSL 763733Egi SugiantoNoch keine Bewertungen
- S. No. ID Full Name Father's Name State DistrictDokument183 SeitenS. No. ID Full Name Father's Name State DistrictManoj ARNoch keine Bewertungen
- Read Ebook America Bewitched: The Story of Witchcraft After Salem by Owen Davies EPUB, AZW, DOC, MOBIDokument2 SeitenRead Ebook America Bewitched: The Story of Witchcraft After Salem by Owen Davies EPUB, AZW, DOC, MOBIkavitazNoch keine Bewertungen
- Valentine Angel MelanieDokument40 SeitenValentine Angel MelanieSarita E Schz100% (6)
- A Beginners Guide To D&D Magic UsersDokument10 SeitenA Beginners Guide To D&D Magic UsersminifezNoch keine Bewertungen
- My Presentation FrameDokument36 SeitenMy Presentation FrameKamal Luitel100% (1)
- Muscles Functions Exercises Pictures: 2. Biceps (Elbow Flexors)Dokument5 SeitenMuscles Functions Exercises Pictures: 2. Biceps (Elbow Flexors)Spongie BobNoch keine Bewertungen