Das könnte Ihnen auch gefallen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- PharmDos LAB - M2.2Dokument7 SeitenPharmDos LAB - M2.2Gianna LingadNoch keine Bewertungen
- UniKL MESTECH Hosts A Public Lecture by DR Ben Forbes From King's College LondonDokument1 SeiteUniKL MESTECH Hosts A Public Lecture by DR Ben Forbes From King's College LondonHuda NazriNoch keine Bewertungen
- (BLUE PACOP) Pharmaceutical Jurisprudence & EthicsDokument31 Seiten(BLUE PACOP) Pharmaceutical Jurisprudence & EthicsDenise Yanci Demiar100% (1)
- Access Corporate Fact SheetDokument2 SeitenAccess Corporate Fact SheetMattNoch keine Bewertungen
- AHM 540 - Merged DocumentDokument429 SeitenAHM 540 - Merged DocumentKanishka KartikeyaNoch keine Bewertungen
- Stockleys 12e - 9780857113474 PDFDokument1 SeiteStockleys 12e - 9780857113474 PDFPark arima67% (3)
- Ebook Pharmacotherapy Principles and Practice Sixth Edition PDF Full Chapter PDFDokument67 SeitenEbook Pharmacotherapy Principles and Practice Sixth Edition PDF Full Chapter PDFmerlin.mitchell336100% (22)
- Hard Gelatin Capsules Today - and TomorrowDokument23 SeitenHard Gelatin Capsules Today - and TomorrowsamxuNoch keine Bewertungen
- HealthTech v17-1Dokument65 SeitenHealthTech v17-1Vansh AggarwalNoch keine Bewertungen
- Community Health Alliance 2018-2019 Annual ReportDokument12 SeitenCommunity Health Alliance 2018-2019 Annual ReportCommunity Health Alliance NevadaNoch keine Bewertungen
- 2021 CCNExamCandidateHandbook Chisholp PlaceDokument12 Seiten2021 CCNExamCandidateHandbook Chisholp PlaceMeriNoch keine Bewertungen
- DR Ashfaq ResumeDokument1 SeiteDR Ashfaq Resumedidoba7635Noch keine Bewertungen
- 〈1160〉 PHARMACEUTICAL CALCULATIONS IN PHARMACY PRACTICEDokument27 Seiten〈1160〉 PHARMACEUTICAL CALCULATIONS IN PHARMACY PRACTICEAptkeluarga SastraNoch keine Bewertungen
- Remdesivir Injection 100 MG Pharmacy Manual v2 March 2020Dokument15 SeitenRemdesivir Injection 100 MG Pharmacy Manual v2 March 2020Gurpreet SinghNoch keine Bewertungen
- Goa India 483 PDFDokument38 SeitenGoa India 483 PDFAnkur ChoudharyNoch keine Bewertungen
- SCM Final PPT PresentationDokument15 SeitenSCM Final PPT PresentationHassan KhanNoch keine Bewertungen
- Rb801 Rasashastra and Bhaishajya Kalpana - I 4-0-0-4Dokument6 SeitenRb801 Rasashastra and Bhaishajya Kalpana - I 4-0-0-4sillypoloNoch keine Bewertungen
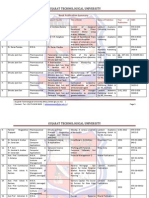
- Book Publication SummaryDokument34 SeitenBook Publication Summaryenggeng7Noch keine Bewertungen
- CS 3075593948Dokument3 SeitenCS 3075593948DantiNoch keine Bewertungen
- Daftar Harga Tiap PBFDokument4 SeitenDaftar Harga Tiap PBFPraja Setia NingsihNoch keine Bewertungen
- New Product Priority List For Development - Oct 2020Dokument46 SeitenNew Product Priority List For Development - Oct 2020GaFf ArNoch keine Bewertungen
- 10 PG Standard Treatment Guidelines Final 08Dokument24 Seiten10 PG Standard Treatment Guidelines Final 08yosafat mustikoartoNoch keine Bewertungen
- Oral Solid Dosage FormsDokument58 SeitenOral Solid Dosage FormsMitul ShahNoch keine Bewertungen
- Formulation and Evaluation of Sublingual Tablets oDokument6 SeitenFormulation and Evaluation of Sublingual Tablets oRindyani AgustinaNoch keine Bewertungen
- Drugs Enquiry Committee (D.E.C), 1930Dokument10 SeitenDrugs Enquiry Committee (D.E.C), 1930Venkata Sai Kiran GudisevaNoch keine Bewertungen
- Apprenticeship Agreement - Student-IPGDokument1 SeiteApprenticeship Agreement - Student-IPGOnche AbrahamNoch keine Bewertungen
- Pharmaceutics-1-Bp103t-2021 Question PaperDokument1 SeitePharmaceutics-1-Bp103t-2021 Question PaperazeosysNoch keine Bewertungen
- Degree CollegesDokument11 SeitenDegree CollegesRohit JainNoch keine Bewertungen
- AntibioticsDokument1 SeiteAntibioticshellionNoch keine Bewertungen
- Yellow Card Spontaneous MonitoringDokument34 SeitenYellow Card Spontaneous Monitoringpavan_baggaNoch keine Bewertungen