Das könnte Ihnen auch gefallen
- Tuli Mnedadak ncbiDokument6 SeitenTuli Mnedadak ncbiMiss AmyNoch keine Bewertungen
- Vol 54 No 2 Patel Selby YekkiralaDokument5 SeitenVol 54 No 2 Patel Selby YekkiralaDrashua AshuaNoch keine Bewertungen
- Small Fiber Neuropathy and Related Syndromes: Pain and NeurodegenerationVon EverandSmall Fiber Neuropathy and Related Syndromes: Pain and NeurodegenerationSung-Tsang HsiehNoch keine Bewertungen
- International Journal of Pediatric OtorhinolaryngologyDokument4 SeitenInternational Journal of Pediatric OtorhinolaryngologyDear Farah SielmaNoch keine Bewertungen
- Agostini 2016 - The Prevention of EpilepsyDokument2 SeitenAgostini 2016 - The Prevention of EpilepsyMark CheongNoch keine Bewertungen
- Status Epilepticus in Adults: A Study From Nigeria: SciencedirectDokument6 SeitenStatus Epilepticus in Adults: A Study From Nigeria: SciencedirectLuther ThengNoch keine Bewertungen
- Presentasi Kasus Sudden Deafness Dhana 2017Dokument9 SeitenPresentasi Kasus Sudden Deafness Dhana 2017Pradhana FwNoch keine Bewertungen
- 01 WNL 0000042787 51461 d1Dokument2 Seiten01 WNL 0000042787 51461 d1veronikiNoch keine Bewertungen
- BPPV Vs SSNHLDokument4 SeitenBPPV Vs SSNHLDicky FebriantoNoch keine Bewertungen
- Jurnal ReadingDokument27 SeitenJurnal ReadingPatresya LantanNoch keine Bewertungen
- Infectious Dan Autoantibody Associated EncephalitisDokument13 SeitenInfectious Dan Autoantibody Associated EncephalitisAyudiah ParamitaNoch keine Bewertungen
- Parinaud Syndrome: Any Clinicoradiological Correlation?: L. Pollak - T. Zehavi-Dorin - A. Eyal - R. Milo - R. Huna-BaronDokument6 SeitenParinaud Syndrome: Any Clinicoradiological Correlation?: L. Pollak - T. Zehavi-Dorin - A. Eyal - R. Milo - R. Huna-BaronJessica HerreraNoch keine Bewertungen
- Late-Onset Rasmussen's Encephalitis and Long-Term Remission: Clinical CommentaryDokument4 SeitenLate-Onset Rasmussen's Encephalitis and Long-Term Remission: Clinical CommentarySana ShafeeqNoch keine Bewertungen
- Red and Orange Flags For Secondary Headache (SNOOP 10)Dokument11 SeitenRed and Orange Flags For Secondary Headache (SNOOP 10)rizkiNoch keine Bewertungen
- Glossopharyngeal Nerve Injury Following Tonsillectomy 5542Dokument4 SeitenGlossopharyngeal Nerve Injury Following Tonsillectomy 5542Kenza SeddikNoch keine Bewertungen
- Dementia Due To NeurosyphilisDokument3 SeitenDementia Due To NeurosyphilisIOSRjournalNoch keine Bewertungen
- Burden of Dizziness and Vertigo in The CommunityDokument8 SeitenBurden of Dizziness and Vertigo in The CommunityEcaterina ChiriacNoch keine Bewertungen
- The NORSE (New-Onset Refractory Status Epileptic Us) SyndromeDokument4 SeitenThe NORSE (New-Onset Refractory Status Epileptic Us) Syndromebenghooi75Noch keine Bewertungen
- Case Report: Vertigo As A Predominant Manifestation of NeurosarcoidosisDokument5 SeitenCase Report: Vertigo As A Predominant Manifestation of NeurosarcoidosisDjumadi AkbarNoch keine Bewertungen
- Prevalence of Idiopathic Normal Pressure Hydrocephalus: A Prospective, Population-Based StudyDokument11 SeitenPrevalence of Idiopathic Normal Pressure Hydrocephalus: A Prospective, Population-Based StudyNovrianda Eka PutraNoch keine Bewertungen
- Neurosyphilis: The Reemergence of An Historical DiseaseDokument2 SeitenNeurosyphilis: The Reemergence of An Historical DiseaseDrashua AshuaNoch keine Bewertungen
- The Successful Treatment of DisinhibitioDokument4 SeitenThe Successful Treatment of DisinhibitioVicky NotesNoch keine Bewertungen
- Case Report: A Case of Herpes Simplex Virus-1 Encephalitis From A Medicolegal Point of ViewDokument4 SeitenCase Report: A Case of Herpes Simplex Virus-1 Encephalitis From A Medicolegal Point of Viewzefri suhendarNoch keine Bewertungen
- Clinical Reasoning: A Young Man With Recurrent Paralysis, Revisable White Matter Lesions and Peripheral Neuropathy Word Count: 945Dokument13 SeitenClinical Reasoning: A Young Man With Recurrent Paralysis, Revisable White Matter Lesions and Peripheral Neuropathy Word Count: 945aileenzhongNoch keine Bewertungen
- Sudden Deafness 2Dokument8 SeitenSudden Deafness 2Aldhi Putra PradanaNoch keine Bewertungen
- Acute Hypotonia in An Infant (2017)Dokument3 SeitenAcute Hypotonia in An Infant (2017)nikos.alexandrNoch keine Bewertungen
- Acute Unilateral Vestibulopathy Strupp & Magnusson (2015)Dokument17 SeitenAcute Unilateral Vestibulopathy Strupp & Magnusson (2015)J WNoch keine Bewertungen
- Neurology and Neurotherapy: ClinmedDokument4 SeitenNeurology and Neurotherapy: ClinmedChristian Hasudungan NainggolanNoch keine Bewertungen
- Approach To HeadacheDokument61 SeitenApproach To Headachesabahat.husainNoch keine Bewertungen
- Algoritmo en UrgenciasDokument9 SeitenAlgoritmo en UrgenciasJulioNoch keine Bewertungen
- Optic Chiasmatic-Hypothalamic Glioma TreatmentDokument1 SeiteOptic Chiasmatic-Hypothalamic Glioma TreatmentLise Westergaard-NeuNoch keine Bewertungen
- Diagnosis Tolosa HuntDokument7 SeitenDiagnosis Tolosa HuntHedy AngelineNoch keine Bewertungen
- Visual Evoked Potentials in Guillain-Barré Syndrome: MethodsDokument6 SeitenVisual Evoked Potentials in Guillain-Barré Syndrome: MethodsYulianti PurnamasariNoch keine Bewertungen
- Fneur 08 00507Dokument8 SeitenFneur 08 00507bozasnachoNoch keine Bewertungen
- Meningoencephalitis and New Onset of Seizures in A Patient With Normal Brain CT and Multiple Lesions On MRIDokument3 SeitenMeningoencephalitis and New Onset of Seizures in A Patient With Normal Brain CT and Multiple Lesions On MRITryas YulithaNoch keine Bewertungen
- Malignant Otitis Externa 20070821Dokument0 SeitenMalignant Otitis Externa 20070821Suci PramadianiNoch keine Bewertungen
- Brain Abscess Case: Drug Abuser with Endocarditis and HemiparesisDokument22 SeitenBrain Abscess Case: Drug Abuser with Endocarditis and HemiparesisAariNoch keine Bewertungen
- A Cohort Study To Assess The New WHO Japanese Encephalitis Surveillance StandardsDokument9 SeitenA Cohort Study To Assess The New WHO Japanese Encephalitis Surveillance StandardsarmankoassracunNoch keine Bewertungen
- Sleep Consult TemplateDokument5 SeitenSleep Consult Templatesbonvallet3912100% (1)
- Status Epileptic in Pediatric PDFDokument12 SeitenStatus Epileptic in Pediatric PDFHanna SimbolonNoch keine Bewertungen
- The Clinical Value of A Thorough Diagnostic Evalua 2019 American Journal ofDokument6 SeitenThe Clinical Value of A Thorough Diagnostic Evalua 2019 American Journal ofGhulam GilmaniNoch keine Bewertungen
- Neuroretinitis Syphilis in Human Immunodeficiency Virus-Infected PatientDokument6 SeitenNeuroretinitis Syphilis in Human Immunodeficiency Virus-Infected PatientAnindya AgrasidiNoch keine Bewertungen
- 6-Diagnosis and Treatment of Nonepileptic Seizures.11Dokument16 Seiten6-Diagnosis and Treatment of Nonepileptic Seizures.11مجاهد إسماعيل حسن حسينNoch keine Bewertungen
- Sleep Hypoventilation in Neuromuscular and Chest Wall DisordersDokument15 SeitenSleep Hypoventilation in Neuromuscular and Chest Wall Disorderssavvy_as_98-1Noch keine Bewertungen
- Santoso 2020Dokument10 SeitenSantoso 2020Aldo VictoriaNoch keine Bewertungen
- Attending Osteomyelitis ModuleDokument9 SeitenAttending Osteomyelitis ModuleMrLarry DolorNoch keine Bewertungen
- Phi RythmDokument6 SeitenPhi RythmStanley IgweNoch keine Bewertungen
- SSNHL EmergensiDokument8 SeitenSSNHL EmergensiYayan AkhyarNoch keine Bewertungen
- Journal of Neuroimmunology: SciencedirectDokument3 SeitenJournal of Neuroimmunology: SciencedirectGrupo 3113 Siglo XXINoch keine Bewertungen
- Sudden Deafness JournalDokument2 SeitenSudden Deafness JournalRestiNoch keine Bewertungen
- Epilepsy: New Advances: Journal ReadingDokument29 SeitenEpilepsy: New Advances: Journal Readingastra yudhaTagamawanNoch keine Bewertungen
- Case Report Tuberculous Otitis MediaDokument23 SeitenCase Report Tuberculous Otitis MediahwelpNoch keine Bewertungen
- Rare Fungal Brain Infection PresentationDokument4 SeitenRare Fungal Brain Infection PresentationmuhammadNoch keine Bewertungen
- Enf Autoinmunes de OidoDokument9 SeitenEnf Autoinmunes de OidomhidvenNoch keine Bewertungen
- Jurnal Reading Saraf ALGIDokument6 SeitenJurnal Reading Saraf ALGIMuhammad Al GifariNoch keine Bewertungen
- Interdisciplinary Neurosurgery: Advanced Techniques and Case ManagementDokument7 SeitenInterdisciplinary Neurosurgery: Advanced Techniques and Case ManagementMuhammad Fuad MahfudNoch keine Bewertungen
- Tinnitus 2019Dokument20 SeitenTinnitus 2019Leslie Lindsay AlvarezNoch keine Bewertungen
- Keys CardiologyDokument1 SeiteKeys CardiologyDrashua AshuaNoch keine Bewertungen
- DM CardiologyDokument39 SeitenDM CardiologyDrashua AshuaNoch keine Bewertungen
- Telephone Directory EngDokument8 SeitenTelephone Directory EngDrashua AshuaNoch keine Bewertungen
- Bihar PG15 ProspectusDokument37 SeitenBihar PG15 ProspectusDrashua AshuaNoch keine Bewertungen
- Post Graduate Medical Admission Test (Pgmat) - 2015 For MD/MS/PGD, MDS & MD (Ayurveda)Dokument2 SeitenPost Graduate Medical Admission Test (Pgmat) - 2015 For MD/MS/PGD, MDS & MD (Ayurveda)Drashua AshuaNoch keine Bewertungen
- Muscle Origins and InsertionsDokument9 SeitenMuscle Origins and Insertionsnoisytaost92% (12)
- Post Graduate Medical Admission Test (Pgmat) - 2014 For MD/MS/PGD, MDS & MD (Ayurveda)Dokument1 SeitePost Graduate Medical Admission Test (Pgmat) - 2014 For MD/MS/PGD, MDS & MD (Ayurveda)Drashua AshuaNoch keine Bewertungen
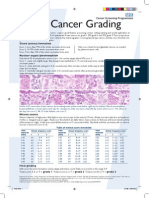
- Breast Cancer Grading PDFDokument1 SeiteBreast Cancer Grading PDFDrashua AshuaNoch keine Bewertungen
- Bence Jones Protein-UrineDokument16 SeitenBence Jones Protein-UrineDrashua Ashua100% (2)
- Post Graduate Medical Admission Test (Pgmat) - 2015 For MD/MS/PGD, MDS & MD (Ayurveda)Dokument2 SeitenPost Graduate Medical Admission Test (Pgmat) - 2015 For MD/MS/PGD, MDS & MD (Ayurveda)Drashua AshuaNoch keine Bewertungen
- Bio Medical Rules PDFDokument28 SeitenBio Medical Rules PDFDrashua AshuaNoch keine Bewertungen
- Compliance rate study of bio-medical waste segregationDokument50 SeitenCompliance rate study of bio-medical waste segregationAman Dheer Kapoor100% (2)
- ABO in The Context ofDokument21 SeitenABO in The Context ofDrashua AshuaNoch keine Bewertungen
- CBD FullDokument5 SeitenCBD FullDrashua AshuaNoch keine Bewertungen
- Hilgendorf Bio 07Dokument52 SeitenHilgendorf Bio 07Drashua AshuaNoch keine Bewertungen
- Application PDFDokument2 SeitenApplication PDFDrashua AshuaNoch keine Bewertungen
- SHIGELLOSISDokument1 SeiteSHIGELLOSISDrashua AshuaNoch keine Bewertungen
- HematologyDokument58 SeitenHematologyAchmad DainuriNoch keine Bewertungen
- Shigella BackgroundDokument2 SeitenShigella BackgroundDrashua AshuaNoch keine Bewertungen
- Ecp Shigella InfectionDokument4 SeitenEcp Shigella InfectionDrashua AshuaNoch keine Bewertungen
- P 133-1430Dokument11 SeitenP 133-1430Drashua AshuaNoch keine Bewertungen
- Shigella in Child-Care SettingsDokument2 SeitenShigella in Child-Care SettingsDrashua AshuaNoch keine Bewertungen
- Shige LLDokument7 SeitenShige LLDrashua AshuaNoch keine Bewertungen
- ID 20i2.1Dokument12 SeitenID 20i2.1Drashua AshuaNoch keine Bewertungen
- 420 079 Guideline ShigellosisDokument7 Seiten420 079 Guideline ShigellosisDrashua AshuaNoch keine Bewertungen
- ShigellaDokument2 SeitenShigellaDrashua AshuaNoch keine Bewertungen
- P 133-1430Dokument11 SeitenP 133-1430Drashua AshuaNoch keine Bewertungen
- Shigellosis: Frequently Asked QuestionsDokument2 SeitenShigellosis: Frequently Asked QuestionsDrashua AshuaNoch keine Bewertungen
- ShigellaDokument1 SeiteShigellaDrashua AshuaNoch keine Bewertungen
- 0314Dokument6 Seiten0314Drashua AshuaNoch keine Bewertungen
- SCDPH Mass COVID19 Vaccination PlanDokument32 SeitenSCDPH Mass COVID19 Vaccination PlanNewsTeam20100% (1)
- Florence Nightingale's Environmental TheoryDokument10 SeitenFlorence Nightingale's Environmental TheoryMANLANGIT, Bianca Trish A.Noch keine Bewertungen
- Nature - Bipolar DisordersDokument16 SeitenNature - Bipolar DisordersVanessa LealNoch keine Bewertungen
- Republic Act No. 10747 (Rare Diseases Act of The Philippines) 2016Dokument8 SeitenRepublic Act No. 10747 (Rare Diseases Act of The Philippines) 2016John Edward Kenneth Macawili RagazaNoch keine Bewertungen
- Pathfit 1 Module 2.1Dokument25 SeitenPathfit 1 Module 2.1James DetallaNoch keine Bewertungen
- Gr9 HP 19 Health TriangleDokument21 SeitenGr9 HP 19 Health TriangleLorraine CalderonNoch keine Bewertungen
- IPHS Fo SC PHC CHCDokument18 SeitenIPHS Fo SC PHC CHCDrArun SinghNoch keine Bewertungen
- CESAR AUGUSTO GALVEZ - Biblical Perspective On Health For The Contemporary WorldDokument11 SeitenCESAR AUGUSTO GALVEZ - Biblical Perspective On Health For The Contemporary WorldDanielNoch keine Bewertungen
- Nursing Process 1Dokument19 SeitenNursing Process 1Anonymous zBblKD8gvNoch keine Bewertungen
- Supportive Cancer Care PDFDokument346 SeitenSupportive Cancer Care PDFtri windartiNoch keine Bewertungen
- 1000 English Collocations in 10 Minutes A DayDokument128 Seiten1000 English Collocations in 10 Minutes A DayThanh TuyenNoch keine Bewertungen
- Testing For COVID-19Dokument2 SeitenTesting For COVID-19oanaNoch keine Bewertungen
- Wollo University College of Medicine and Health Scince Department of PhrmacyDokument16 SeitenWollo University College of Medicine and Health Scince Department of Phrmacynegussie birieNoch keine Bewertungen
- How to live a healthy lifestyleDokument8 SeitenHow to live a healthy lifestyleAbdul Rahim JaafarNoch keine Bewertungen
- ARI Varmam Therapy Mail Today Article 25jan 2011Dokument1 SeiteARI Varmam Therapy Mail Today Article 25jan 2011Arts Research InstituteNoch keine Bewertungen
- Report On Community Health DiagnosisDokument118 SeitenReport On Community Health DiagnosisRubina Pulami100% (15)
- Divine Intervention Episode 36 Usmle OphthalmologyDokument15 SeitenDivine Intervention Episode 36 Usmle OphthalmologySwisskelly1Noch keine Bewertungen
- CoopMED Health Insurance Doctor Examination FormDokument2 SeitenCoopMED Health Insurance Doctor Examination FormKammieNoch keine Bewertungen
- Health Needs Assessment StepsDokument40 SeitenHealth Needs Assessment Stepsdennis8113100% (2)
- Portfolio explores genius, obstacles and medical decisionsDokument15 SeitenPortfolio explores genius, obstacles and medical decisionsSofia Patricia Salazar AllccacoNoch keine Bewertungen
- Introduction To Community Health NursingDokument54 SeitenIntroduction To Community Health NursingNestor CabacunganNoch keine Bewertungen
- Franco Gera Hi An 93356145 Ethics EssayDokument13 SeitenFranco Gera Hi An 93356145 Ethics EssayFranco GerahianNoch keine Bewertungen
- Stress and Immune SystemDokument15 SeitenStress and Immune SystemRhishabhNoch keine Bewertungen
- IPHSDokument95 SeitenIPHSprabha krishnan100% (1)
- IVF Access for Cystic Fibrosis PatientsDokument13 SeitenIVF Access for Cystic Fibrosis PatientsUpasana GurunathanNoch keine Bewertungen
- EMOTIONAL and Behavioral DisordersDokument3 SeitenEMOTIONAL and Behavioral Disordersjonacambri06Noch keine Bewertungen
- Comprehensive Development Plan for the City of San Fernando, PampangaDokument153 SeitenComprehensive Development Plan for the City of San Fernando, PampangaPopoy CanlapanNoch keine Bewertungen
- Scope and Sequence in MapehDokument14 SeitenScope and Sequence in MapehVerna M. Reyes100% (2)
- NCP - Alcohol AbuseDokument2 SeitenNCP - Alcohol AbuseJerome GazmenNoch keine Bewertungen
- Biochemistry of Aging Lab OutlineDokument1 SeiteBiochemistry of Aging Lab OutlineKeila RosalesNoch keine Bewertungen