Das könnte Ihnen auch gefallen
- COVID-19 Vaccination PlanDokument46 SeitenCOVID-19 Vaccination PlanFOX 17 NewsNoch keine Bewertungen
- Teaching and Learning ResourcesDokument4 SeitenTeaching and Learning ResourcesTey Lee PohNoch keine Bewertungen
- MathsDokument27 SeitenMathsBA21412Noch keine Bewertungen
- Astm A182Dokument2 SeitenAstm A182fastenersworldNoch keine Bewertungen
- Managing Immunization ProgramsDokument24 SeitenManaging Immunization Programskristine ezpeletaNoch keine Bewertungen
- Clinical Mentorship in Public Health SettingsDokument58 SeitenClinical Mentorship in Public Health Settingshappyraam0% (1)
- Primary Checkpoint - Science (0846) October 2016 Paper 2 MSDokument12 SeitenPrimary Checkpoint - Science (0846) October 2016 Paper 2 MSdinakarc78% (9)
- Essentials of Report Writing - Application in BusinessDokument28 SeitenEssentials of Report Writing - Application in BusinessMahmudur Rahman75% (4)
- Early Cancer Detection in Primary Care: Are You Aware of New Blood-Based Multi-Cancer Screening ToolsVon EverandEarly Cancer Detection in Primary Care: Are You Aware of New Blood-Based Multi-Cancer Screening ToolsNoch keine Bewertungen
- Data Science From Scratch, 2nd EditionDokument72 SeitenData Science From Scratch, 2nd EditionAhmed HusseinNoch keine Bewertungen
- MCQ Part 1 2005 "Example Questions"Dokument3 SeitenMCQ Part 1 2005 "Example Questions"RayC1977Noch keine Bewertungen
- The Fifth DisciplineDokument15 SeitenThe Fifth DisciplineZau Seng50% (2)
- Monitoring, Evaluating, and Improving: An Evidence-Based Approach to Achieving Development Results that Matter!Von EverandMonitoring, Evaluating, and Improving: An Evidence-Based Approach to Achieving Development Results that Matter!Noch keine Bewertungen
- National Tuberculosis Control Program Manual of Procedures 5th EditionDokument192 SeitenNational Tuberculosis Control Program Manual of Procedures 5th EditionBlue Pielago100% (9)
- PQ of Vial Washer Ensures Removal of ContaminantsDokument25 SeitenPQ of Vial Washer Ensures Removal of ContaminantsJuan DanielNoch keine Bewertungen
- Strategies For Dengue Control ProgramDokument22 SeitenStrategies For Dengue Control ProgramNaseem QaziNoch keine Bewertungen
- Combination HIV Prevention: Tailoring Programs To Stop TransmissionDokument2 SeitenCombination HIV Prevention: Tailoring Programs To Stop TransmissionFuturesGroup1Noch keine Bewertungen
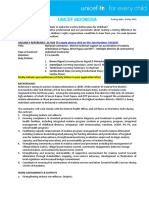
- Unicef Indonesia: Vacancy Reference: 21-024 (Dokument3 SeitenUnicef Indonesia: Vacancy Reference: 21-024 (Ina LabokNoch keine Bewertungen
- Combination HIV Prevention: Tailoring Programs To Stop TransmissionDokument2 SeitenCombination HIV Prevention: Tailoring Programs To Stop TransmissionFuturesGroup1Noch keine Bewertungen
- MSF Medical M&E Coordinator RoleDokument3 SeitenMSF Medical M&E Coordinator RoleMyo Thant ZinNoch keine Bewertungen
- Building Capacity For Universal Coverage: Malaria Control in NigeriaDokument28 SeitenBuilding Capacity For Universal Coverage: Malaria Control in Nigeriamalaria_consortiumNoch keine Bewertungen
- ReportingDokument2 SeitenReportingStephanie Dela CruzNoch keine Bewertungen
- Global Malaria Action PlanDokument30 SeitenGlobal Malaria Action PlanhjsagdNoch keine Bewertungen
- Project Axshya (The Union)Dokument2 SeitenProject Axshya (The Union)curiouscrollNoch keine Bewertungen
- VR-23-022 National Consultant Malaria Elimination - 230614 - 080708Dokument3 SeitenVR-23-022 National Consultant Malaria Elimination - 230614 - 080708kucing9956Noch keine Bewertungen
- Clinton Health Access Initiative Conference PosterDokument1 SeiteClinton Health Access Initiative Conference PosterNathan WilkinsonNoch keine Bewertungen
- Annex I National Leprosy Eradication ProgrammeDokument5 SeitenAnnex I National Leprosy Eradication ProgrammespmdocNoch keine Bewertungen
- SEA Region's Continuity of TB Services During Covid-19Dokument44 SeitenSEA Region's Continuity of TB Services During Covid-19Muhamad JenNoch keine Bewertungen
- Adv CommDokument6 SeitenAdv CommK SNoch keine Bewertungen
- Nurses' Knowledge On Nosocomial Infections Preventive Measures and Its Associated Factors in Ghana A Cross-Sectional Study BMDokument1 SeiteNurses' Knowledge On Nosocomial Infections Preventive Measures and Its Associated Factors in Ghana A Cross-Sectional Study BMahilhamza55Noch keine Bewertungen
- Manyati-Mutsau2021 Article ExploringTheEffectivenessOfTelDokument8 SeitenManyati-Mutsau2021 Article ExploringTheEffectivenessOfTelInformationTechnology ConsultingGroupNoch keine Bewertungen
- Raw 2 LawsDokument17 SeitenRaw 2 LawsRed HaleNoch keine Bewertungen
- Vacancy No.: Date:: 31 October 2020Dokument3 SeitenVacancy No.: Date:: 31 October 2020thanNoch keine Bewertungen
- Utures Roup Urope: Service AreasDokument2 SeitenUtures Roup Urope: Service AreasFuturesGroup1Noch keine Bewertungen
- Islands of Tuberculosis Elimination: An Evaluation of Community-Based Active Case Finding in North Sumatra, IndonesiaDokument12 SeitenIslands of Tuberculosis Elimination: An Evaluation of Community-Based Active Case Finding in North Sumatra, IndonesiaRahmadika NofriNoch keine Bewertungen
- Project Design Document - Model Answers-RAG ProjectDokument19 SeitenProject Design Document - Model Answers-RAG ProjectGis ThaNoch keine Bewertungen
- STP-T ConceptNote 0 enDokument34 SeitenSTP-T ConceptNote 0 enHarari Management and Kaizen Institute (HMKI)Noch keine Bewertungen
- Embargoed - Covid-19 Vaccination Plan 10-21-20Dokument40 SeitenEmbargoed - Covid-19 Vaccination Plan 10-21-20WJHL News Channel ElevenNoch keine Bewertungen
- 2013 NTP MOP Chapter 8 ACSM 12apr2014Dokument28 Seiten2013 NTP MOP Chapter 8 ACSM 12apr2014Vanessa Devota Veloso - RamirezNoch keine Bewertungen
- P R Echpp: Puerto Rico Enhanced Comprehensive Hiv Prevention Plan (Prechpp)Dokument4 SeitenP R Echpp: Puerto Rico Enhanced Comprehensive Hiv Prevention Plan (Prechpp)almanaque2011Noch keine Bewertungen
- Evaluation of Aedes-Borne Disease Prevention ProgramDokument4 SeitenEvaluation of Aedes-Borne Disease Prevention ProgramBARBARA ALLY ZAMORANoch keine Bewertungen
- Partnering With The Global Fund: Who Global TB ProgrammeDokument2 SeitenPartnering With The Global Fund: Who Global TB ProgrammeLawlit L Al GhifariNoch keine Bewertungen
- TB PosterDokument13 SeitenTB Posterthamizhselvi87Noch keine Bewertungen
- Policy Brief - Aid and Accountability in Sierra Leone's Health Sector and Mechanisms For Effectiveness FinalDokument4 SeitenPolicy Brief - Aid and Accountability in Sierra Leone's Health Sector and Mechanisms For Effectiveness FinalAnsumana MusaNoch keine Bewertungen
- VN - Technical Support To The TB Response in The Philippines Amid The COVID 19 Pandemic and The Transition Towards UHCDokument5 SeitenVN - Technical Support To The TB Response in The Philippines Amid The COVID 19 Pandemic and The Transition Towards UHCJeane Irish EgotNoch keine Bewertungen
- AfricaProgramForOncho APOCDokument2 SeitenAfricaProgramForOncho APOCAbdulkader TukaleNoch keine Bewertungen
- GESI - From NACO - CleanDokument35 SeitenGESI - From NACO - CleanMatin Ahmad KhanNoch keine Bewertungen
- Community Dialogues For Healthy Children: Encouraging Communities To TalkDokument32 SeitenCommunity Dialogues For Healthy Children: Encouraging Communities To Talkmalaria_consortiumNoch keine Bewertungen
- 14.6aids Control ProgrammeDokument9 Seiten14.6aids Control Programmevenkat krishnanNoch keine Bewertungen
- Country Progress ReportDokument19 SeitenCountry Progress Reportprk1234Noch keine Bewertungen
- Reviewed Annual Report Hiv - FinalDokument43 SeitenReviewed Annual Report Hiv - FinalGretchen VenturaNoch keine Bewertungen
- Mdast Final Report Aug 2013 Printed VersionDokument41 SeitenMdast Final Report Aug 2013 Printed VersionEmmanuel Peter KulwaNoch keine Bewertungen
- 1dublin Declaration Hiv Data Evidence BriefDokument3 Seiten1dublin Declaration Hiv Data Evidence BriefFrancisca BallesterosNoch keine Bewertungen
- Abstract Linkage of CAST TB Cases To Care in Nabilatuk DistrictDokument1 SeiteAbstract Linkage of CAST TB Cases To Care in Nabilatuk Districtakena raymonedNoch keine Bewertungen
- Determinants of Facility Readiness For Integration of Family Planning With HIV Testing and Counseling Services: Evidence From The Tanzania Service Provision Assessment Survey, 2014 - 2015Dokument11 SeitenDeterminants of Facility Readiness For Integration of Family Planning With HIV Testing and Counseling Services: Evidence From The Tanzania Service Provision Assessment Survey, 2014 - 2015yuliaNoch keine Bewertungen
- TOR - Medical OfficerDokument3 SeitenTOR - Medical OfficernewarakanNoch keine Bewertungen
- 72570336malaria KambojaDokument12 Seiten72570336malaria KambojaArum Ayu KartikaNoch keine Bewertungen
- Amref Health Africa - New VacanciesDokument10 SeitenAmref Health Africa - New VacanciesAdelina MwageniNoch keine Bewertungen
- Pacific Convergence Paper1Dokument45 SeitenPacific Convergence Paper1rizzakayeNoch keine Bewertungen
- The Global Fund's New Funding Model: Early Outcomes For Regional Civil Society ApplicantsDokument15 SeitenThe Global Fund's New Funding Model: Early Outcomes For Regional Civil Society ApplicantsKataisee RichardsonNoch keine Bewertungen
- C11 P07 National Aids Control ProgrammeDokument32 SeitenC11 P07 National Aids Control ProgrammeChandana KrishnaNoch keine Bewertungen
- National Policy and Strategic Plan of Action On Non-Communicable Diseases (NCDS)Dokument6 SeitenNational Policy and Strategic Plan of Action On Non-Communicable Diseases (NCDS)Lawal AwofiranyeNoch keine Bewertungen
- Surveillance, forecasting and response to reduce healthcare associated infectionsDokument1 SeiteSurveillance, forecasting and response to reduce healthcare associated infectionszenagit123456Noch keine Bewertungen
- NPO NOB - HIV & Care TreatmentDokument3 SeitenNPO NOB - HIV & Care TreatmentAnabay MamoNoch keine Bewertungen
- TB Prev CTRL Program 4.5.2021Dokument123 SeitenTB Prev CTRL Program 4.5.2021JeslineNoch keine Bewertungen
- JC3085E - Community Led Monitoring in Action - enDokument48 SeitenJC3085E - Community Led Monitoring in Action - engoncalves.mariopauloNoch keine Bewertungen
- Strengthening Coherence between Agriculture and Social Protection to Combat Poverty and Hunger in Africa Diagnostic ToolVon EverandStrengthening Coherence between Agriculture and Social Protection to Combat Poverty and Hunger in Africa Diagnostic ToolNoch keine Bewertungen
- Meeting the Needs of Older Adults with Serious Illness: Challenges and Opportunities in the Age of Health Care ReformVon EverandMeeting the Needs of Older Adults with Serious Illness: Challenges and Opportunities in the Age of Health Care ReformAmy S. KelleyNoch keine Bewertungen
- Flashcard TemplateDokument1 SeiteFlashcard TemplateRayC1977Noch keine Bewertungen
- Flashcard TemplateDokument1 SeiteFlashcard TemplateRayC1977Noch keine Bewertungen
- FC Path (SA) Anat Part I Past Papers - 2020 1st Semester 18 2 2020Dokument2 SeitenFC Path (SA) Anat Part I Past Papers - 2020 1st Semester 18 2 2020RayC1977Noch keine Bewertungen
- Drivers of Quality in TB Control in South African Correctional FacilitiesDokument1 SeiteDrivers of Quality in TB Control in South African Correctional FacilitiesRayC1977Noch keine Bewertungen
- Environments. Therefore, Phenomenon Such As Self-Fulfilling Prophecies, Enactment andDokument1 SeiteEnvironments. Therefore, Phenomenon Such As Self-Fulfilling Prophecies, Enactment andRayC1977Noch keine Bewertungen
- Hydroponics SummaryDokument4 SeitenHydroponics SummaryJose NovoaNoch keine Bewertungen
- A-00 IndexDokument10 SeitenA-00 IndexNizarHamrouniNoch keine Bewertungen
- Name: Chakshu Purohit Course: BBA LLB Subject: Legal Research and Methodology Submitted To: Utkarsh MishraDokument5 SeitenName: Chakshu Purohit Course: BBA LLB Subject: Legal Research and Methodology Submitted To: Utkarsh Mishrachakshu purohitNoch keine Bewertungen
- Procedure For NC and CapaDokument2 SeitenProcedure For NC and CapaSAKTHIVEL ANoch keine Bewertungen
- Ground Floor 40X80 Option-1Dokument1 SeiteGround Floor 40X80 Option-1Ashish SrivastavaNoch keine Bewertungen
- Effects of Zero Moment of Truth On Consumer Behavior For FMCGDokument14 SeitenEffects of Zero Moment of Truth On Consumer Behavior For FMCGBoogii EnkhboldNoch keine Bewertungen
- ListDokument4 SeitenListgeralda pierrelusNoch keine Bewertungen
- Adjectives Weekly Plan1Dokument10 SeitenAdjectives Weekly Plan1RItta MariaNoch keine Bewertungen
- Uvas CaractDokument10 SeitenUvas CaractgondeluNoch keine Bewertungen
- Coca Cola Live-ProjectDokument20 SeitenCoca Cola Live-ProjectKanchan SharmaNoch keine Bewertungen
- Attribute Achievement FormDokument15 SeitenAttribute Achievement FormMiguel MenesesNoch keine Bewertungen
- Organized Educator Seeks New OpportunityDokument1 SeiteOrganized Educator Seeks New OpportunityCaren Pogoy ManiquezNoch keine Bewertungen
- PENGARUH CYBERBULLYING BODY SHAMING TERHADAP KEPERCAYAAN DIRIDokument15 SeitenPENGARUH CYBERBULLYING BODY SHAMING TERHADAP KEPERCAYAAN DIRIRizky Hizrah WumuNoch keine Bewertungen
- Ôn tập và kiểm tra học kì Tiếng anh 6 ĐÁP ÁNDokument143 SeitenÔn tập và kiểm tra học kì Tiếng anh 6 ĐÁP ÁNThùy TinaNoch keine Bewertungen
- Facebook TemplateDokument2 SeitenFacebook Templateapi-352106462Noch keine Bewertungen
- BS en 1044-1999 - Brazing Filler MetalsDokument26 SeitenBS en 1044-1999 - Brazing Filler MetalsBorn ToSinNoch keine Bewertungen
- Key Personnel'S Affidavit of Commitment To Work On The ContractDokument14 SeitenKey Personnel'S Affidavit of Commitment To Work On The ContractMica BisaresNoch keine Bewertungen
- Parts of A Computer With Their FunctionsDokument19 SeitenParts of A Computer With Their FunctionsJaried SumbaNoch keine Bewertungen
- Introduction To Machine Learning Top-Down Approach - Towards Data ScienceDokument6 SeitenIntroduction To Machine Learning Top-Down Approach - Towards Data ScienceKashaf BakaliNoch keine Bewertungen
- User Manual - Rev3Dokument31 SeitenUser Manual - Rev3SyahdiNoch keine Bewertungen
- Mumbai Tourist Attractions.Dokument2 SeitenMumbai Tourist Attractions.Guru SanNoch keine Bewertungen
- Valhalla Repair ManualDokument8 SeitenValhalla Repair ManualKirby AllenNoch keine Bewertungen
- M Audio bx10s Manuel Utilisateur en 27417Dokument8 SeitenM Audio bx10s Manuel Utilisateur en 27417TokioNoch keine Bewertungen