Das könnte Ihnen auch gefallen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Claims & Billing Submission GuidelinesDokument93 SeitenClaims & Billing Submission GuidelinesbilalakNoch keine Bewertungen
- Federal Benefits Open Season Highlights 2023 Plan YearDokument12 SeitenFederal Benefits Open Season Highlights 2023 Plan YearFedSmith Inc.100% (1)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- WBDG Hospitals & Care HomesDokument394 SeitenWBDG Hospitals & Care Homesaqua2376Noch keine Bewertungen
- Morse Fall ScaleDokument2 SeitenMorse Fall Scalesidekick941100% (1)
- Head NursingDokument4 SeitenHead NursingJan Ong100% (5)
- Dr. Beckett Case StudyDokument9 SeitenDr. Beckett Case StudyJhay QuiazonNoch keine Bewertungen
- PhilHealth Circ2017-0003Dokument6 SeitenPhilHealth Circ2017-0003Toche DoceNoch keine Bewertungen
- Cme Fluid and Electrolytes 2902016Dokument37 SeitenCme Fluid and Electrolytes 2902016Mohd Faie Ramli0% (1)
- Housemanship Officer Rotation DataDokument1 SeiteHousemanship Officer Rotation DataMohd Faie RamliNoch keine Bewertungen
- Principles of FractureDokument32 SeitenPrinciples of FractureMohd Faie RamliNoch keine Bewertungen
- Fix FR Tibia FibulaDokument33 SeitenFix FR Tibia FibulaMohd Faie RamliNoch keine Bewertungen
- Final Fantasy IVDokument221 SeitenFinal Fantasy IVMohd Faie RamliNoch keine Bewertungen
- Textbook Compartment Syndrome FixDokument18 SeitenTextbook Compartment Syndrome FixMohd Faie Ramli100% (1)
- Critical Care Management of Severe Traumatic Brain Injury in AdultsDokument15 SeitenCritical Care Management of Severe Traumatic Brain Injury in AdultsMohd Faie RamliNoch keine Bewertungen
- STL 15 5Dokument8 SeitenSTL 15 5Mohd Faie RamliNoch keine Bewertungen
- TGADokument9 SeitenTGAMohd Faie RamliNoch keine Bewertungen
- Patch TestDokument10 SeitenPatch TestMartin GaniNoch keine Bewertungen
- TGVDokument4 SeitenTGVMohd Faie RamliNoch keine Bewertungen
- Svark Health Atm - ResidentialsDokument16 SeitenSvark Health Atm - Residentialssanjeevsharma28Noch keine Bewertungen
- August 17, 2012 Strathmore TimesDokument28 SeitenAugust 17, 2012 Strathmore TimesStrathmore TimesNoch keine Bewertungen
- Apollo Reach - Affordable Healthcare - Case StudyDokument7 SeitenApollo Reach - Affordable Healthcare - Case StudyyogiesharmaNoch keine Bewertungen
- 2008 AnnualDokument100 Seiten2008 AnnualKori PratiwiNoch keine Bewertungen
- Wellstar Cobb Hospital: Implementation StrategyDokument32 SeitenWellstar Cobb Hospital: Implementation StrategywuddafrenNoch keine Bewertungen
- FRSA Flash January 18thDokument14 SeitenFRSA Flash January 18thjenblossom1981Noch keine Bewertungen
- Improving The Care of Older Adults Full ReportDokument74 SeitenImproving The Care of Older Adults Full ReportKhoirun NisyakNoch keine Bewertungen
- Cricket Academy Head Coach RoleDokument4 SeitenCricket Academy Head Coach Roletauseef1716Noch keine Bewertungen
- Quality Improvement ProjectDokument6 SeitenQuality Improvement Projectapi-317112346Noch keine Bewertungen
- PPE AuditTool PDFDokument1 SeitePPE AuditTool PDFARIKANoch keine Bewertungen
- Diabetic Keywordio Longtail KeywordsDokument12 SeitenDiabetic Keywordio Longtail KeywordsVic HNNoch keine Bewertungen
- AP - Hospital Wise ReportDokument11 SeitenAP - Hospital Wise ReportKumarNoch keine Bewertungen
- Change Pays.: Cowboy Music RevueDokument1 SeiteChange Pays.: Cowboy Music RevueTIRNoch keine Bewertungen
- 5 Highest Paid Employees of Maines Largest HospitalsDokument1 Seite5 Highest Paid Employees of Maines Largest HospitalsPattie ReavesNoch keine Bewertungen
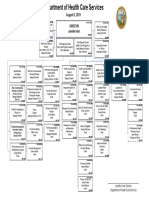
- Department of Health Care Services organizational chartDokument1 SeiteDepartment of Health Care Services organizational chartpedro perezNoch keine Bewertungen
- Digital Healthcare White PaperDokument63 SeitenDigital Healthcare White PapersteverubisNoch keine Bewertungen
- Carpenter IndictmentDokument7 SeitenCarpenter IndictmentToby Harper0% (1)
- Hospital To Hospital Transfers Marina Rivers April 12Dokument12 SeitenHospital To Hospital Transfers Marina Rivers April 12Flossie SingletonNoch keine Bewertungen
- 1500 Health Insurance Claim Form 02 - 12 Revised PDF OWENDokument2 Seiten1500 Health Insurance Claim Form 02 - 12 Revised PDF OWENtonyaNoch keine Bewertungen
- Group 9 - Cambridge HospitalDokument10 SeitenGroup 9 - Cambridge HospitalJahja0% (1)
- Bedah Jurnal Case ManagementDokument1 SeiteBedah Jurnal Case ManagementpusriwatyNoch keine Bewertungen
- HIPAA Web Course Test AnswersDokument4 SeitenHIPAA Web Course Test AnswersMokeshdharan RNoch keine Bewertungen
- Making Sense of Social Prescribing 2017Dokument79 SeitenMaking Sense of Social Prescribing 2017Gail WardNoch keine Bewertungen