Das könnte Ihnen auch gefallen
- Mental Health Nursing HandoutDokument27 SeitenMental Health Nursing HandoutKim Ramos100% (26)
- Psychiatric NursingDokument20 SeitenPsychiatric Nursingchio0809100% (4)
- Case Study SchizophreniaDokument3 SeitenCase Study SchizophreniaCHRISANTO ARZANANNoch keine Bewertungen
- Lecture Notes For Mental Health Nursing Psych NursingDokument88 SeitenLecture Notes For Mental Health Nursing Psych Nursingjg369097100% (1)
- Psychiatric Nursing 2Dokument14 SeitenPsychiatric Nursing 2api-3731845100% (3)
- Psychiatric Nursing NotesDokument12 SeitenPsychiatric Nursing NotesKarla FralalaNoch keine Bewertungen
- Psych Drugs NursingDokument7 SeitenPsych Drugs Nursinglisa100% (2)
- Final Exam Review Sheet1 Mental Health NursingDokument20 SeitenFinal Exam Review Sheet1 Mental Health NursingStephanie Talbot100% (56)
- Energy Psychology - GalloDokument285 SeitenEnergy Psychology - GalloMDB100% (5)
- Chapter 2 - Neurobiologic Theories and PsychopharmacologyDokument11 SeitenChapter 2 - Neurobiologic Theories and PsychopharmacologyCatia FernandesNoch keine Bewertungen
- Anatomy of AnxietyDokument3 SeitenAnatomy of AnxietykhnumdumandfullofcumNoch keine Bewertungen
- Psychiatric NursingDokument20 SeitenPsychiatric NursingRI NA100% (1)
- Mental IllnessDokument60 SeitenMental IllnessAnneNicoleMirtoCorderoNoch keine Bewertungen
- Chapter 24 Cognitive DisordersDokument7 SeitenChapter 24 Cognitive DisordersCatia Fernandes100% (1)
- Psych Nursing CompleteDokument31 SeitenPsych Nursing CompletebajaocNoch keine Bewertungen
- Borderline Personality DisorderDokument17 SeitenBorderline Personality DisorderKirstie de LunaNoch keine Bewertungen
- Maladaptive Patterns of BehaviorDokument186 SeitenMaladaptive Patterns of Behaviorjackyd5100% (1)
- Psych Student NotesDokument23 SeitenPsych Student NotesReymund Timog TalarocNoch keine Bewertungen
- Understand Your Child's Anxiety: What Is Worry?Dokument8 SeitenUnderstand Your Child's Anxiety: What Is Worry?Sanja ZupaničNoch keine Bewertungen
- Psychiatric Nursing FCDokument8 SeitenPsychiatric Nursing FCdhodejunlNoch keine Bewertungen
- Psychiatric Test BankDokument67 SeitenPsychiatric Test BankHABEI KWODI100% (1)
- Psychiatric Nursing ReviewDokument27 SeitenPsychiatric Nursing Reviewgrey26Noch keine Bewertungen
- Mnemonics and Tips Related To Psychiatric NursingDokument2 SeitenMnemonics and Tips Related To Psychiatric NursingDr. Jayesh Patidar100% (1)
- Psych NotesDokument24 SeitenPsych NotesMae Ann Flores Mahinay100% (2)
- LearnFM Clinical Card Book 2020Dokument67 SeitenLearnFM Clinical Card Book 2020Aqilah Syafiqah100% (1)
- Nursing Process in Psychiatric NursingDokument11 SeitenNursing Process in Psychiatric Nursinglissa_permataNoch keine Bewertungen
- Chapter 11 Anger, Hostility, and AggressionDokument4 SeitenChapter 11 Anger, Hostility, and AggressionCatia Fernandes100% (1)
- Practice Test Psychiatric Nursing 150 ItemsDokument24 SeitenPractice Test Psychiatric Nursing 150 ItemsPaul Christian P. Santos, RN93% (40)
- Psychiatric and MentalDokument16 SeitenPsychiatric and MentalJanine Garcia100% (2)
- Additional Nursing Care Plans - SchizophreniaDokument26 SeitenAdditional Nursing Care Plans - SchizophreniaJasmin Jacob100% (5)
- Review Notes For Psychiatric NursingDokument75 SeitenReview Notes For Psychiatric Nursinglisette_sakuraNoch keine Bewertungen
- Anxiety DisordersDokument18 SeitenAnxiety DisordersAzahed ArturoNoch keine Bewertungen
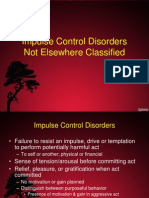
- Impulse Control DisordersDokument97 SeitenImpulse Control DisordersGanpat VankarNoch keine Bewertungen
- NCM 117 - Nurse Patient Interaction - April 2021Dokument58 SeitenNCM 117 - Nurse Patient Interaction - April 2021kimberly dedaseNoch keine Bewertungen
- Psychiatric and Mental Health Nursing Practice TestDokument9 SeitenPsychiatric and Mental Health Nursing Practice Testjeshema45% (11)
- Psyche Eval 1Dokument6 SeitenPsyche Eval 1KimTot OctavianoNoch keine Bewertungen
- Psychosocial Care of Older Adults: Cognition and Perception: Ma. Concepcion A. Maico, RN, MAN, Ed.DDokument35 SeitenPsychosocial Care of Older Adults: Cognition and Perception: Ma. Concepcion A. Maico, RN, MAN, Ed.DMEJIE MARL RAVEN INSTRELLANoch keine Bewertungen
- Videbeck Psychiatric Mental Health Nursing Chapter Work SheetDokument46 SeitenVidebeck Psychiatric Mental Health Nursing Chapter Work SheetYannah Mae Espineli100% (1)
- PowerPoint Presentation To Accompany Videbeck's Psychiatric Mental Health NursingDokument18 SeitenPowerPoint Presentation To Accompany Videbeck's Psychiatric Mental Health NursingDennis James BartolomeNoch keine Bewertungen
- Nursing Process in Psychiatric NursingDokument14 SeitenNursing Process in Psychiatric NursingJomark Palgan100% (1)
- NCM 117 - Psychiatric Nursing (MODULE 1 & 2)Dokument8 SeitenNCM 117 - Psychiatric Nursing (MODULE 1 & 2)Meryville JacildoNoch keine Bewertungen
- Basic Concepts in Psychiatric NursingDokument11 SeitenBasic Concepts in Psychiatric NursingMae DacerNoch keine Bewertungen
- Mental Health Nursing Case StudyDokument9 SeitenMental Health Nursing Case Studyapi-454984300Noch keine Bewertungen
- Medical Surgical Nursing Review 1Dokument422 SeitenMedical Surgical Nursing Review 1jeshemaNoch keine Bewertungen
- 50 Item Psychiatric Exam Answers and RationalesDokument9 Seiten50 Item Psychiatric Exam Answers and RationalesJune DumdumayaNoch keine Bewertungen
- Comprehensive Exam NCM 145Dokument17 SeitenComprehensive Exam NCM 145Adrian Dela CruzNoch keine Bewertungen
- Psychiatric Nurse: Passbooks Study GuideVon EverandPsychiatric Nurse: Passbooks Study GuideNoch keine Bewertungen
- Chapter 18 Personality DisordersDokument10 SeitenChapter 18 Personality DisordersCatia Fernandes100% (2)
- Sterile - : Definition of TermsDokument8 SeitenSterile - : Definition of TermsEdson John DemayoNoch keine Bewertungen
- Chapter 4 Treatment Settings and Theraputic PRogramsDokument5 SeitenChapter 4 Treatment Settings and Theraputic PRogramsCatia Fernandes100% (1)
- PMH Nursing Care Plan 01112017Dokument19 SeitenPMH Nursing Care Plan 01112017api-371817203Noch keine Bewertungen
- Funda - Pretest 2Dokument10 SeitenFunda - Pretest 2FreeNursingNotesNoch keine Bewertungen
- COMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideVon EverandCOMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideNoch keine Bewertungen
- De-Escalating Agressive PatientDokument48 SeitenDe-Escalating Agressive PatientAbelNoch keine Bewertungen
- Crisis Intervention: Srinivasan ADokument12 SeitenCrisis Intervention: Srinivasan AsrinivasanaNoch keine Bewertungen
- AngerHostility and AggressionDokument32 SeitenAngerHostility and AggressionKathreen TamayoNoch keine Bewertungen
- Topic 7 Theories of CounselingDokument114 SeitenTopic 7 Theories of Counselingdicksandayo8Noch keine Bewertungen
- SchizophreniaDokument45 SeitenSchizophreniasinuaish syaNoch keine Bewertungen
- PD NotesDokument9 SeitenPD Notesmely dela cruzNoch keine Bewertungen
- Adjustment Disorder and Defence MechanismDokument51 SeitenAdjustment Disorder and Defence MechanismMarvellousNoch keine Bewertungen
- Psychological Responses To Medical DisordersDokument51 SeitenPsychological Responses To Medical DisordersShikhaNoch keine Bewertungen
- Personality Disorder Unit 6Dokument29 SeitenPersonality Disorder Unit 6Gulshad AfridiNoch keine Bewertungen
- A Male Client With Dementia Often Assaults The NursingDokument15 SeitenA Male Client With Dementia Often Assaults The NursingchaSeph100% (4)
- LowdermilkDokument46 SeitenLowdermilkMishi BajwaNoch keine Bewertungen
- Personality DisordersDokument99 SeitenPersonality DisordersdanesarosebNoch keine Bewertungen
- Major Depressive DisorderDokument23 SeitenMajor Depressive DisorderYeng Cries100% (1)
- Miranda-Castillo Et Al. - 2019 - Validation of The Geriatric Anxiety Inventory in Chilean Older PeopleDokument20 SeitenMiranda-Castillo Et Al. - 2019 - Validation of The Geriatric Anxiety Inventory in Chilean Older PeoplePaulina Negrón DíazNoch keine Bewertungen
- 3-Anxiety DisordersDokument57 Seiten3-Anxiety DisordersVidya BalaNoch keine Bewertungen
- Panic Disorder - Etiology & Clinical FeaturesDokument49 SeitenPanic Disorder - Etiology & Clinical Featuresdrkadiyala2Noch keine Bewertungen
- Table 5-8 - DSM-5 Diagnostic Criteria For Panic DisorderDokument1 SeiteTable 5-8 - DSM-5 Diagnostic Criteria For Panic DisorderDragutin PetrićNoch keine Bewertungen
- Mental Health Promotion in SchoolsDokument19 SeitenMental Health Promotion in SchoolsAaron VillegasNoch keine Bewertungen
- Crim IIIDokument16 SeitenCrim IIILoubert AbiertaNoch keine Bewertungen
- The Worry Wars:: Equipping Our Child Clients To Effectively Fight Their FearsDokument16 SeitenThe Worry Wars:: Equipping Our Child Clients To Effectively Fight Their FearsAngeliki HoNoch keine Bewertungen
- A Review of Literature of Anxiety Amongst AdolescenceDokument3 SeitenA Review of Literature of Anxiety Amongst AdolescenceViveca Isabelle NamiaNoch keine Bewertungen
- ContinueDokument3 SeitenContinueojasvibatraNoch keine Bewertungen
- English Investigatory ProjectDokument15 SeitenEnglish Investigatory Projectdevlopmentoverhere001Noch keine Bewertungen
- Perinatal Mood and Anxiety Disorders: What Are They?Dokument2 SeitenPerinatal Mood and Anxiety Disorders: What Are They?Maranda BartschiNoch keine Bewertungen
- Fear of Public SpeakingDokument16 SeitenFear of Public SpeakingSerc YablaNoch keine Bewertungen
- Baas Et Al., (2017)Dokument12 SeitenBaas Et Al., (2017)Andrea BarrosoNoch keine Bewertungen
- The Development of Anxiety Disorders: Considering The Contributions of Attachment and Emotion RegulationDokument15 SeitenThe Development of Anxiety Disorders: Considering The Contributions of Attachment and Emotion RegulationJohannes CordeNoch keine Bewertungen
- Abpsy 3rd Exam ReviewerDokument7 SeitenAbpsy 3rd Exam ReviewerJusa Aldrea PratoNoch keine Bewertungen
- Jarricot Dermatome Pain Test Validation As A DiagnosticDokument9 SeitenJarricot Dermatome Pain Test Validation As A DiagnosticJesus BrownNoch keine Bewertungen
- Mental Health Literacy and Anxiety Disorder PDFDokument11 SeitenMental Health Literacy and Anxiety Disorder PDFShabrina Patriavy BennaradictaNoch keine Bewertungen
- Makaylee Fowler - AnxietyDokument4 SeitenMakaylee Fowler - Anxietyapi-589524812Noch keine Bewertungen
- Introduction To Abnormal Child and Adolescent Psychology 3Rd Full ChapterDokument41 SeitenIntroduction To Abnormal Child and Adolescent Psychology 3Rd Full Chapterjames.popp962100% (19)
- How To Get Help For HypochondriaDokument8 SeitenHow To Get Help For HypochondriaWasim RashidNoch keine Bewertungen
- Sperling - The Role of Intolerance of Uncertainty in Treatment For Pediatric Anxiety Disorders and Obsessive-Compulsive DisorderDokument11 SeitenSperling - The Role of Intolerance of Uncertainty in Treatment For Pediatric Anxiety Disorders and Obsessive-Compulsive DisorderMonika ZikraNoch keine Bewertungen
- Literature Review Anxiety DisorderDokument5 SeitenLiterature Review Anxiety Disordervrxhvexgf100% (1)
- Northeastern Mindanao CollegesDokument58 SeitenNortheastern Mindanao CollegesGliese Grace BuhiaNoch keine Bewertungen
- Mental Health and Academic Performance of First-Year College StudentsDokument10 SeitenMental Health and Academic Performance of First-Year College StudentsANoch keine Bewertungen