Das könnte Ihnen auch gefallen
- Course Outline:: Basic Accounting Principles and Financial ConceptsDokument2 SeitenCourse Outline:: Basic Accounting Principles and Financial ConceptsAr JayNoch keine Bewertungen
- Format of ReportDokument3 SeitenFormat of ReportAr JayNoch keine Bewertungen
- Region II Trauma Center Monthly Consumption ReportDokument2 SeitenRegion II Trauma Center Monthly Consumption ReportAr JayNoch keine Bewertungen
- List of Quality IndicatorsDokument2 SeitenList of Quality IndicatorsAr JayNoch keine Bewertungen
- CSC SPMS PDFDokument56 SeitenCSC SPMS PDFAr JayNoch keine Bewertungen
- Daily Performance Output ReportDokument5 SeitenDaily Performance Output ReportAr JayNoch keine Bewertungen
- Medical Supply Monitoring SheetDokument3 SeitenMedical Supply Monitoring SheetAr JayNoch keine Bewertungen
- Census Remark Code Task Q E T: Surgical Intensive Care UnitDokument1 SeiteCensus Remark Code Task Q E T: Surgical Intensive Care UnitAr JayNoch keine Bewertungen
- Medical and Office Equipment Fuctionality Monitoring SheetDokument3 SeitenMedical and Office Equipment Fuctionality Monitoring SheetAr JayNoch keine Bewertungen
- Emergency Drug Monitoring SheetDokument3 SeitenEmergency Drug Monitoring SheetAr JayNoch keine Bewertungen
- Form Daily Individual Performance Management ChecklistDokument4 SeitenForm Daily Individual Performance Management ChecklistAr JayNoch keine Bewertungen
- Level III Evaluation - Behavioral LevelDokument2 SeitenLevel III Evaluation - Behavioral LevelAr JayNoch keine Bewertungen
- PArts Please PrintDokument1 SeitePArts Please PrintAr JayNoch keine Bewertungen
- CompetencyDokument7 SeitenCompetencyAr JayNoch keine Bewertungen
- List of Quality IndicatorsDokument2 SeitenList of Quality IndicatorsAr JayNoch keine Bewertungen
- Infection Control RiskDokument2 SeitenInfection Control RiskAr JayNoch keine Bewertungen
- CSC SPMS PDFDokument56 SeitenCSC SPMS PDFAr JayNoch keine Bewertungen
- Civil Service VRH Iso Petu: (As Individual Staff Nurse/ Midwife/ Nursing Attendant) (As A Unit/Section/Ward) (As A Nurse)Dokument1 SeiteCivil Service VRH Iso Petu: (As Individual Staff Nurse/ Midwife/ Nursing Attendant) (As A Unit/Section/Ward) (As A Nurse)Ar JayNoch keine Bewertungen
- b1 FinelliDokument42 Seitenb1 FinelliAr JayNoch keine Bewertungen
- Ipcr Kabisote Ob orDokument2 SeitenIpcr Kabisote Ob orAr JayNoch keine Bewertungen
- Introductory Article - OPDDokument1 SeiteIntroductory Article - OPDAr JayNoch keine Bewertungen
- Com-Spms Form No. 3 (Ipcr) : (Please Add Rows If Necessary)Dokument3 SeitenCom-Spms Form No. 3 (Ipcr) : (Please Add Rows If Necessary)Ar Jay100% (13)
- Department of SurgeryDokument2 SeitenDepartment of SurgeryAr Jay100% (1)
- Quality IndicatorsDokument152 SeitenQuality IndicatorsAr JayNoch keine Bewertungen
- Etoshow QuityDokument8 SeitenEtoshow QuityAr JayNoch keine Bewertungen
- Surgical Intensive Care Unit-Nuerovital Signs Monitoring ToolDokument1 SeiteSurgical Intensive Care Unit-Nuerovital Signs Monitoring ToolAr JayNoch keine Bewertungen
- Quality IndicatorsDokument45 SeitenQuality IndicatorsAr JayNoch keine Bewertungen
- Assessing A PatientDokument1 SeiteAssessing A PatientAr JayNoch keine Bewertungen
- Rheumatic Heart DiseaseDokument21 SeitenRheumatic Heart DiseaseAr JayNoch keine Bewertungen
- Give Psychological Support To The Patient and FamilyDokument2 SeitenGive Psychological Support To The Patient and FamilyNílo StárnNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Urology ST3 Portfolio Self-Assessment Guidance 2018Dokument6 SeitenUrology ST3 Portfolio Self-Assessment Guidance 2018kaNoch keine Bewertungen
- Robert G. Gish, MD Full Curriculum Vitae & Biography - Updated January 2015Dokument231 SeitenRobert G. Gish, MD Full Curriculum Vitae & Biography - Updated January 2015Robert G. Gish, MDNoch keine Bewertungen
- Orthopedic Surgery Complete IMG ListDokument153 SeitenOrthopedic Surgery Complete IMG ListF AbdullaNoch keine Bewertungen
- Regulations and Rules For MRCPCH and DCH ExaminationsDokument18 SeitenRegulations and Rules For MRCPCH and DCH ExaminationsSyed Danish AliNoch keine Bewertungen
- INICET July 22 Result MDMS - MDS For WebsiteDokument565 SeitenINICET July 22 Result MDMS - MDS For WebsiteSwetha pugazhNoch keine Bewertungen
- UntitledDokument955 SeitenUntitledمزاجية المودNoch keine Bewertungen
- MCQ Sin Medical Physiology 1Dokument2 SeitenMCQ Sin Medical Physiology 1priyaNoch keine Bewertungen
- Faculty Registration Details HistoryDokument3 SeitenFaculty Registration Details HistorySunny Kashyap0% (1)
- List of Candidates Selected For PG DEGREE /DIPLOMA / 6yr M.Ch. (NEURO SURGERY) 2012 - 2013 SESSION ON 16/05/2012Dokument7 SeitenList of Candidates Selected For PG DEGREE /DIPLOMA / 6yr M.Ch. (NEURO SURGERY) 2012 - 2013 SESSION ON 16/05/2012Reuben JosephNoch keine Bewertungen
- Health Family Welfare 3Dokument225 SeitenHealth Family Welfare 3Gopala Sundararaj SNoch keine Bewertungen
- Final Govt MD Ms PG Dip Mds 2016Dokument37 SeitenFinal Govt MD Ms PG Dip Mds 2016rahulNoch keine Bewertungen
- PIMS AICET PG II BrochureDokument53 SeitenPIMS AICET PG II BrochureAnweshaBoseNoch keine Bewertungen
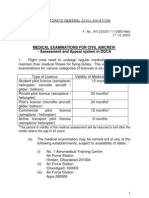
- Medical - Appeal Procedure DGCADokument6 SeitenMedical - Appeal Procedure DGCAБисвас АнупамNoch keine Bewertungen
- Ed 304 Catiag FinalDokument34 SeitenEd 304 Catiag FinalDEXTER LLOYD CATIAGNoch keine Bewertungen
- Booklet For PHMC (Revised)Dokument24 SeitenBooklet For PHMC (Revised)Govt Ayurvedic Teaching Hospital WarangalNoch keine Bewertungen
- ASTMH Diploma Course List 8 - 19Dokument10 SeitenASTMH Diploma Course List 8 - 19saurabh pandeyNoch keine Bewertungen
- Self-Reported Dental Student Stressors and ExperiencesDokument8 SeitenSelf-Reported Dental Student Stressors and ExperiencesVíctor RodríguezNoch keine Bewertungen
- Full Download Ebook Ebook PDF Nelson Essentials of Pediatrics 8th Edition PDFDokument41 SeitenFull Download Ebook Ebook PDF Nelson Essentials of Pediatrics 8th Edition PDFdavid.anderson198100% (37)
- Obstetricia y Ginecología Beckman 8a EdicionDokument477 SeitenObstetricia y Ginecología Beckman 8a EdicionAlejandro Mora100% (2)
- ProspectusDokument52 SeitenProspectusRabinder BakhshiNoch keine Bewertungen
- The Malaysian Qualifications Framework PDFDokument39 SeitenThe Malaysian Qualifications Framework PDFDsgSyedNasRul100% (1)
- Physical Medicine & Rehabilitation - Randall BraddomDokument1.482 SeitenPhysical Medicine & Rehabilitation - Randall BraddomSimona Chirică90% (10)
- EndocrinologyDokument31 SeitenEndocrinologyDevi VaraNoch keine Bewertungen
- Critical Care of Children With Heart Disease 2010Dokument735 SeitenCritical Care of Children With Heart Disease 2010Haikel Mhamed100% (1)
- Orthopaedic Rehabilitation of The Athlete Getting Back in Game 1st Edition Ebook PDF VersionDokument62 SeitenOrthopaedic Rehabilitation of The Athlete Getting Back in Game 1st Edition Ebook PDF Versionkevin.smart540100% (42)
- Xavier BrochureDokument20 SeitenXavier BrochureJohn PareraNoch keine Bewertungen
- Avery's Diseases of The Newborn, Eleventh Edition - 2024Dokument1.849 SeitenAvery's Diseases of The Newborn, Eleventh Edition - 2024Brillence M SammyNoch keine Bewertungen
- DME AP Recruitment 2021 Notification For 326 Assistant Professor Posts Apply OnlineDokument6 SeitenDME AP Recruitment 2021 Notification For 326 Assistant Professor Posts Apply OnlineRajesh K KumarNoch keine Bewertungen
- Neuropsychology in IndiaDokument16 SeitenNeuropsychology in IndiaRahula RakeshNoch keine Bewertungen
- Doctors Blank CV TemplateDokument10 SeitenDoctors Blank CV TemplateMostafa ElkaramanyNoch keine Bewertungen