Das könnte Ihnen auch gefallen
- Facial AnatomyDokument11 SeitenFacial AnatomySneha SthaNoch keine Bewertungen
- Evoked PotentialDokument6 SeitenEvoked PotentialVikas VatsNoch keine Bewertungen
- Alternative Method For Fabrication of Power ArmDokument2 SeitenAlternative Method For Fabrication of Power ArmVikas VatsNoch keine Bewertungen
- Vestibuloplasty With Skin Grafting and Lowering of The-HandoutDokument6 SeitenVestibuloplasty With Skin Grafting and Lowering of The-HandoutVikas VatsNoch keine Bewertungen
- Pikos-Mandibluar Block Autografts For Alveolar Ridge AugmentationDokument17 SeitenPikos-Mandibluar Block Autografts For Alveolar Ridge AugmentationVikas VatsNoch keine Bewertungen
- BJOMS 2011. Technical Note. Use of Methylene Blue For Precise Peripheral Ostectomy of Keratocystic Odontogenic TumourDokument2 SeitenBJOMS 2011. Technical Note. Use of Methylene Blue For Precise Peripheral Ostectomy of Keratocystic Odontogenic TumourVikas Vats100% (1)
- HN 03-2011 Submadibular Salivary Gland Transfer PDFDokument7 SeitenHN 03-2011 Submadibular Salivary Gland Transfer PDFVikas VatsNoch keine Bewertungen
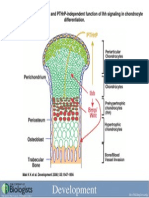
- Development 2008 Jun 135 (11) 1947-56, Fig. 7.Dokument1 SeiteDevelopment 2008 Jun 135 (11) 1947-56, Fig. 7.Vikas VatsNoch keine Bewertungen
- Computer-Assisted Navigational Surgery in Oral and Maxillofacial SurgeryDokument9 SeitenComputer-Assisted Navigational Surgery in Oral and Maxillofacial SurgeryVikas VatsNoch keine Bewertungen
- 1545 1569 (2000) 037 0243:amouof 2.3.co 2Dokument5 Seiten1545 1569 (2000) 037 0243:amouof 2.3.co 2Vikas VatsNoch keine Bewertungen
- Rhinoplasty Dissection ManualDokument185 SeitenRhinoplasty Dissection ManualVikas Vats100% (3)
- Acute Effects of Radiation InjuryDokument8 SeitenAcute Effects of Radiation InjuryVikas VatsNoch keine Bewertungen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Subject Manual Tle 7-8Dokument11 SeitenSubject Manual Tle 7-8Rhayan Dela Cruz DaquizNoch keine Bewertungen
- PresentationDokument27 SeitenPresentationMenuka WatankachhiNoch keine Bewertungen
- Catify To Satisfy - Simple Solutions For Creating A Cat-Friendly Home (PDFDrive)Dokument315 SeitenCatify To Satisfy - Simple Solutions For Creating A Cat-Friendly Home (PDFDrive)Paz Libros100% (2)
- (1921) Manual of Work Garment Manufacture: How To Improve Quality and Reduce CostsDokument102 Seiten(1921) Manual of Work Garment Manufacture: How To Improve Quality and Reduce CostsHerbert Hillary Booker 2nd100% (1)
- How He Loves PDFDokument2 SeitenHow He Loves PDFJacob BullockNoch keine Bewertungen
- Implementation of E-Governance To Improve The Civil Administration Service Quality in Public SectorDokument11 SeitenImplementation of E-Governance To Improve The Civil Administration Service Quality in Public SectorChristie YohanaNoch keine Bewertungen
- Kyle Pape - Between Queer Theory and Native Studies, A Potential For CollaborationDokument16 SeitenKyle Pape - Between Queer Theory and Native Studies, A Potential For CollaborationRafael Alarcón Vidal100% (1)
- Radon-222 Exhalation From Danish Building Material PDFDokument63 SeitenRadon-222 Exhalation From Danish Building Material PDFdanpalaciosNoch keine Bewertungen
- Kazon Greater Predator MothershipDokument1 SeiteKazon Greater Predator MothershipknavealphaNoch keine Bewertungen
- Cooperative Learning: Complied By: ANGELICA T. ORDINEZADokument16 SeitenCooperative Learning: Complied By: ANGELICA T. ORDINEZAAlexis Kaye GullaNoch keine Bewertungen
- Thesis PaperDokument53 SeitenThesis PaperAnonymous AOOrehGZAS100% (1)
- Disassembly Procedures: 1 DELL U2422HB - U2422HXBDokument6 SeitenDisassembly Procedures: 1 DELL U2422HB - U2422HXBIonela CristinaNoch keine Bewertungen
- Rajiv Gandhi University of Health Sciences, Bengaluru, KarnatakaDokument9 SeitenRajiv Gandhi University of Health Sciences, Bengaluru, KarnatakaNavin ChandarNoch keine Bewertungen
- Cummin C1100 Fuel System Flow DiagramDokument8 SeitenCummin C1100 Fuel System Flow DiagramDaniel KrismantoroNoch keine Bewertungen
- Acute Appendicitis in Children - Diagnostic Imaging - UpToDateDokument28 SeitenAcute Appendicitis in Children - Diagnostic Imaging - UpToDateHafiz Hari NugrahaNoch keine Bewertungen
- WarringFleets Complete PDFDokument26 SeitenWarringFleets Complete PDFlingshu8100% (1)
- Oxford EAP B1 Pre-Intermediate Student - S Book 2Dokument167 SeitenOxford EAP B1 Pre-Intermediate Student - S Book 2Thư Dương Thị AnhNoch keine Bewertungen
- Delonghi Esam Series Service Info ItalyDokument10 SeitenDelonghi Esam Series Service Info ItalyBrko BrkoskiNoch keine Bewertungen
- Sociology As A Form of Consciousness - 20231206 - 013840 - 0000Dokument4 SeitenSociology As A Form of Consciousness - 20231206 - 013840 - 0000Gargi sharmaNoch keine Bewertungen
- Nanolithography - Processing Methods PDFDokument10 SeitenNanolithography - Processing Methods PDFNilesh BhardwajNoch keine Bewertungen
- Sample Monologues PDFDokument5 SeitenSample Monologues PDFChristina Cannilla100% (1)
- Introduction To Screenwriting UEADokument12 SeitenIntroduction To Screenwriting UEAMartín SalasNoch keine Bewertungen
- Microsmart GEODTU Eng 7Dokument335 SeitenMicrosmart GEODTU Eng 7Jim JonesjrNoch keine Bewertungen
- Assignment of Chemistry For B.sc-B.ed First Semester Session 2019-2023-1Dokument2 SeitenAssignment of Chemistry For B.sc-B.ed First Semester Session 2019-2023-1Payal sahaNoch keine Bewertungen
- Executive Summary-P-5 181.450 To 222Dokument14 SeitenExecutive Summary-P-5 181.450 To 222sat palNoch keine Bewertungen
- Quarter 1 - Module 1Dokument31 SeitenQuarter 1 - Module 1Roger Santos Peña75% (4)
- Comparison Between CompetitorsDokument2 SeitenComparison Between Competitorsritesh singhNoch keine Bewertungen
- Safety Procedures in Using Hand Tools and EquipmentDokument12 SeitenSafety Procedures in Using Hand Tools and EquipmentJan IcejimenezNoch keine Bewertungen
- Week-3-Q1-Gen Chem-Sep-11-15-DllDokument12 SeitenWeek-3-Q1-Gen Chem-Sep-11-15-DllJennette BelliotNoch keine Bewertungen
- QuexBook TutorialDokument14 SeitenQuexBook TutorialJeffrey FarillasNoch keine Bewertungen