Das könnte Ihnen auch gefallen
- Sample SoapDokument9 SeitenSample SoapDouglas Greg Cook90% (20)
- MB0042-MBA-1st Sem 2011 Assignment Managerial EconomicsDokument11 SeitenMB0042-MBA-1st Sem 2011 Assignment Managerial EconomicsAli Asharaf Khan100% (3)
- Farmer Hospitalized with Left-Sided WeaknessDokument13 SeitenFarmer Hospitalized with Left-Sided WeaknessGidu SaidNoch keine Bewertungen
- EM Case Write UpDokument11 SeitenEM Case Write UpRaihana Rafi100% (2)
- Soap Note 5 Acute - Alyssa MatulichDokument7 SeitenSoap Note 5 Acute - Alyssa Matulichapi-456313554Noch keine Bewertungen
- Chronic Diseases - Lymes, Hpv, Hsv Mis-Diagnosis and Mistreatment: A New Approach to the EpidemicVon EverandChronic Diseases - Lymes, Hpv, Hsv Mis-Diagnosis and Mistreatment: A New Approach to the EpidemicBewertung: 5 von 5 Sternen5/5 (1)
- Constitutional: General Appearance: Healthy-Appearing, Well-Nourished, and Well-Developed. Level ofDokument10 SeitenConstitutional: General Appearance: Healthy-Appearing, Well-Nourished, and Well-Developed. Level ofRichard ObinwankwoNoch keine Bewertungen
- 2019 IL and Federal Pharmacy Law Review PDFDokument176 Seiten2019 IL and Federal Pharmacy Law Review PDFAnonymous 3YNJfYNQ100% (5)
- Pedia 1Dokument8 SeitenPedia 1Jani MisterioNoch keine Bewertungen
- Sample Write UpDokument2 SeitenSample Write UpNar Patrick Padilla100% (1)
- Final Assessment Soap NoteDokument13 SeitenFinal Assessment Soap Noteapi-494643478100% (3)
- CVA Case PresentationDokument16 SeitenCVA Case PresentationgolokipokNoch keine Bewertungen
- Nurs 5018 - Soap Note Well-Woman ExamDokument7 SeitenNurs 5018 - Soap Note Well-Woman Examapi-308904543Noch keine Bewertungen
- Health Assessment Project: Name: Ena Lewis Tutor: Sis Francis Group: 15Dokument27 SeitenHealth Assessment Project: Name: Ena Lewis Tutor: Sis Francis Group: 15Blake KamminNoch keine Bewertungen
- PEDIA Case 4.1. Dengue FeverDokument10 SeitenPEDIA Case 4.1. Dengue Feverotartil_nimanNoch keine Bewertungen
- My Son The Fanatic, Short StoryDokument4 SeitenMy Son The Fanatic, Short StoryScribdAddict100% (2)
- CASE 3 MEDICINE JULY 10 2019 AcutePyeloDokument15 SeitenCASE 3 MEDICINE JULY 10 2019 AcutePyeloTrisNoch keine Bewertungen
- Soap 2Dokument5 SeitenSoap 2api-456313554Noch keine Bewertungen
- Seminar 6 Precision AttachmentsDokument30 SeitenSeminar 6 Precision AttachmentsAmit Sadhwani67% (3)
- List of PEGA Interview Questions and AnswersDokument33 SeitenList of PEGA Interview Questions and Answersknagender100% (1)
- Low Back PainDokument9 SeitenLow Back PainDoc AchondoNoch keine Bewertungen
- Case PresentationDokument15 SeitenCase PresentationHarriette Quimby TibucNoch keine Bewertungen
- Facial Edema and Kidney Disease in a 5-Year-Old BoyDokument13 SeitenFacial Edema and Kidney Disease in a 5-Year-Old BoyLuigi FranciscoNoch keine Bewertungen
- Temptations in MinistryDokument115 SeitenTemptations in MinistryJoseph Koech100% (1)
- Jharkhand Steel Casting CompaniesDokument6 SeitenJharkhand Steel Casting CompaniesCatherine Jovita50% (2)
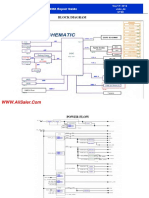
- Asus X553MA Repair Guide Rev2.0Dokument7 SeitenAsus X553MA Repair Guide Rev2.0UMA AKANDU UCHENoch keine Bewertungen
- Template Gyn Lo Abd PainDokument18 SeitenTemplate Gyn Lo Abd PainHassan HarirNoch keine Bewertungen
- SOAP note 1 - Breast CADokument4 SeitenSOAP note 1 - Breast CAacvalvarioNoch keine Bewertungen
- IVMS ICM HX Sample Write-UpDokument4 SeitenIVMS ICM HX Sample Write-UpMarc Imhotep Cray, M.D.Noch keine Bewertungen
- CRVHD Percipitated by IEDokument14 SeitenCRVHD Percipitated by IEKemotherapy LifesucksNoch keine Bewertungen
- Acute PancreatitisDokument7 SeitenAcute PancreatitisPatrick DycocoNoch keine Bewertungen
- Form Health History Documentation: Biographical DataDokument7 SeitenForm Health History Documentation: Biographical DataSandra SanonNoch keine Bewertungen
- Case ReportDokument9 SeitenCase ReportBerhanu DigamoNoch keine Bewertungen
- Annual Exam: 52 YO Male Grocery Receiver with HyperlipidemiaDokument5 SeitenAnnual Exam: 52 YO Male Grocery Receiver with HyperlipidemiaMallory ZaborNoch keine Bewertungen
- Validation #3 Graded Documentation SheetsDokument4 SeitenValidation #3 Graded Documentation SheetsGelsey Gelsinator JianNoch keine Bewertungen
- MED2 Case For DR IALs LectureDokument3 SeitenMED2 Case For DR IALs LectureJanelaAngeliGonzalesPanopioNoch keine Bewertungen
- Head To Toe Write UpDokument3 SeitenHead To Toe Write Upapi-554096544Noch keine Bewertungen
- Genome PaperDokument7 SeitenGenome Paperapi-444163791100% (1)
- Addis Ababa University School of Medicine Department of Gynecology & ObstetricsDokument13 SeitenAddis Ababa University School of Medicine Department of Gynecology & Obstetricspilual tongyikNoch keine Bewertungen
- Addis Ababa University Case Report on 31-Year-Old Woman with Vaginal BleedingDokument12 SeitenAddis Ababa University Case Report on 31-Year-Old Woman with Vaginal BleedingdenekeNoch keine Bewertungen
- Case Report V Internal MedicineDokument14 SeitenCase Report V Internal MedicineGidu SaidNoch keine Bewertungen
- Type The Document Title: Department of Surgery Case Report-IiDokument10 SeitenType The Document Title: Department of Surgery Case Report-IiEyosiyas AbiyNoch keine Bewertungen
- FNP 2 ObesityDokument24 SeitenFNP 2 Obesityapi-554096544Noch keine Bewertungen
- Gerontology Project AssessmentDokument15 SeitenGerontology Project AssessmentBlake KamminNoch keine Bewertungen
- History: O Identifying DataDokument10 SeitenHistory: O Identifying DataJofen Ann Hisoler TangpuzNoch keine Bewertungen
- Lung Cancer with Pleural EffusionsDokument8 SeitenLung Cancer with Pleural EffusionsL4 CLERK - UY, Rhea Andrea F.Noch keine Bewertungen
- IM Gastro FinalDokument10 SeitenIM Gastro FinalIzzyMaxinoNoch keine Bewertungen
- Pedia August 29Dokument4 SeitenPedia August 29Raymund AldabaNoch keine Bewertungen
- Right-sided Weakness: 79-Year-Old Male with HypertensionDokument5 SeitenRight-sided Weakness: 79-Year-Old Male with HypertensionFG ArciagaNoch keine Bewertungen
- Nursing Care Plans for Neurological and Cardiovascular CasesDokument15 SeitenNursing Care Plans for Neurological and Cardiovascular CasesJane FlorendoNoch keine Bewertungen
- History and Physical Notes - Final Report: Service Date: Admit Date: Performing ServiceDokument5 SeitenHistory and Physical Notes - Final Report: Service Date: Admit Date: Performing Servicestarskyhutch0000100% (1)
- Case Report IV Internal MedicineDokument11 SeitenCase Report IV Internal MedicineGidu Said100% (1)
- HPI ExampleDokument4 SeitenHPI ExampleSteveNoch keine Bewertungen
- BPH Sample To Case ReportDokument12 SeitenBPH Sample To Case ReportBirhanu ShiferawNoch keine Bewertungen
- Example Write Up #1: A Patient With Diarrhea: Problem ListDokument8 SeitenExample Write Up #1: A Patient With Diarrhea: Problem ListMaher AltaeeNoch keine Bewertungen
- APH Secondary to Placenta Previa 2Dokument10 SeitenAPH Secondary to Placenta Previa 2sirgute tamratNoch keine Bewertungen
- Case Report III Internal MedicineDokument12 SeitenCase Report III Internal MedicineGidu Said0% (1)
- HISTORY # 1 - PCGH, EchavezDokument11 SeitenHISTORY # 1 - PCGH, EchavezHynne Jhea EchavezNoch keine Bewertungen
- Oniphas Homewoek 2Dokument14 SeitenOniphas Homewoek 2Blake KamminNoch keine Bewertungen
- 6904 Module 1 HistoryDokument3 Seiten6904 Module 1 Historyapi-618492022Noch keine Bewertungen
- History Taking Template For StudentsDokument14 SeitenHistory Taking Template For Studentsx88tydcwb2Noch keine Bewertungen
- Geri SOAPsampleDokument8 SeitenGeri SOAPsampleJacquelineNoch keine Bewertungen
- History No. 2: Group 1-Section ADokument61 SeitenHistory No. 2: Group 1-Section ANikko Ryan C'zare AbalosNoch keine Bewertungen
- Chronic Kidney DiseaseDokument6 SeitenChronic Kidney DiseaseDharshan SivaNoch keine Bewertungen
- Left Breast SwellingDokument10 SeitenLeft Breast SwellingfarahmazlanNoch keine Bewertungen
- Ent Case Report Acute Otitis Media Stage IIIDokument12 SeitenEnt Case Report Acute Otitis Media Stage IIIRem Alfelor100% (1)
- The F Bomb: A Formula for Feeling Fabulous in Your 40s, 50s, and FollowingVon EverandThe F Bomb: A Formula for Feeling Fabulous in Your 40s, 50s, and FollowingNoch keine Bewertungen
- Inguinal Hernia and Hydrocele Diagnosis and Treatment in ChildrenDokument10 SeitenInguinal Hernia and Hydrocele Diagnosis and Treatment in ChildrenShelly Stephanie BintoroNoch keine Bewertungen
- Inguinal Hernia and Hydrocele Diagnosis and Treatment in ChildrenDokument10 SeitenInguinal Hernia and Hydrocele Diagnosis and Treatment in ChildrenShelly Stephanie BintoroNoch keine Bewertungen
- Arm 16 ThumbDokument3 SeitenArm 16 Thumbenes_osmić_1Noch keine Bewertungen
- Cover Lapsus HidrokelDokument1 SeiteCover Lapsus HidrokelShelly Stephanie BintoroNoch keine Bewertungen
- Tehnik Penyusunan StatusDokument7 SeitenTehnik Penyusunan StatusShelly Stephanie BintoroNoch keine Bewertungen
- Jaundice PDFDokument29 SeitenJaundice PDFTahtawi 'Afid' Rifai RidhoNoch keine Bewertungen
- Cover Lapsus HidrokelDokument1 SeiteCover Lapsus HidrokelShelly Stephanie BintoroNoch keine Bewertungen
- Inguinal Hernia and Hydrocele Diagnosis and Treatment in ChildrenDokument10 SeitenInguinal Hernia and Hydrocele Diagnosis and Treatment in ChildrenShelly Stephanie BintoroNoch keine Bewertungen
- Tehnik Penyusunan StatusDokument7 SeitenTehnik Penyusunan StatusShelly Stephanie BintoroNoch keine Bewertungen
- Nervous System HistologyDokument4 SeitenNervous System HistologyShelly Stephanie Bintoro100% (1)
- Tehnik Penyusunan StatusDokument7 SeitenTehnik Penyusunan StatusShelly Stephanie BintoroNoch keine Bewertungen
- Avoid Sharing Private Info in IM ChatsDokument1 SeiteAvoid Sharing Private Info in IM ChatsShelly Stephanie BintoroNoch keine Bewertungen
- Nervous System HistologyDokument4 SeitenNervous System HistologyShelly Stephanie Bintoro100% (1)
- Avoid Sharing Private Info in IM ChatsDokument1 SeiteAvoid Sharing Private Info in IM ChatsShelly Stephanie BintoroNoch keine Bewertungen
- Tendernotice 2Dokument20 SeitenTendernotice 2VIVEK SAININoch keine Bewertungen
- ManuscriptDokument2 SeitenManuscriptVanya QuistoNoch keine Bewertungen
- Security Testing MatDokument9 SeitenSecurity Testing MatLias JassiNoch keine Bewertungen
- Intraoperative Nursing Care GuideDokument12 SeitenIntraoperative Nursing Care GuideDarlyn AmplayoNoch keine Bewertungen
- Rubik Clock Solution 1Dokument2 SeitenRubik Clock Solution 1Ionel PaunNoch keine Bewertungen
- DBIRS SyllabusDokument2 SeitenDBIRS SyllabusAshitosh KadamNoch keine Bewertungen
- Rhetorical Analysis ArticleDokument6 SeitenRhetorical Analysis Articleapi-242472728Noch keine Bewertungen
- Math-149 MatricesDokument26 SeitenMath-149 MatricesKurl Vincent GamboaNoch keine Bewertungen
- Sample of Accident Notification & Investigation ProcedureDokument2 SeitenSample of Accident Notification & Investigation Procedurerajendhar100% (1)
- L P 10Dokument13 SeitenL P 10Bình Minh HoàngNoch keine Bewertungen
- Assignment of A Glass Transition Temperature Using Thermomechanical Analysis: Tension MethodDokument4 SeitenAssignment of A Glass Transition Temperature Using Thermomechanical Analysis: Tension MethodEric GozzerNoch keine Bewertungen
- How To Calibrate OscilloscopeDokument2 SeitenHow To Calibrate OscilloscopeninoNoch keine Bewertungen
- Elements of Ayurveda Daily Routine GuideDokument1 SeiteElements of Ayurveda Daily Routine GuideShivani GargNoch keine Bewertungen
- Active Disturbance Rejection Control For Nonlinear SystemsDokument8 SeitenActive Disturbance Rejection Control For Nonlinear SystemsTrần Việt CườngNoch keine Bewertungen
- De Thi HK 2 Tieng Anh 9 de 2Dokument17 SeitenDe Thi HK 2 Tieng Anh 9 de 2Lê Thu HiềnNoch keine Bewertungen
- SAP SD Course Content PDFDokument4 SeitenSAP SD Course Content PDFshuku03Noch keine Bewertungen
- Acc418 2020 2Dokument3 SeitenAcc418 2020 2faithNoch keine Bewertungen
- Re: Laparoscopic Myomectomy: A Review of Alternatives, Techniques and ControversiesDokument1 SeiteRe: Laparoscopic Myomectomy: A Review of Alternatives, Techniques and ControversiesMayada OsmanNoch keine Bewertungen
- Topic1 Whole NumberDokument22 SeitenTopic1 Whole NumberDayang Siti AishahNoch keine Bewertungen
- PA2 Value and PD2 ValueDokument4 SeitenPA2 Value and PD2 Valueguddu1680Noch keine Bewertungen
- NewTrendsInLeadershipandManagement ArikkokDokument32 SeitenNewTrendsInLeadershipandManagement Arikkoksocofem288Noch keine Bewertungen
- Expt 1 Yarn Formation (Sherley Trash Analyser)Dokument7 SeitenExpt 1 Yarn Formation (Sherley Trash Analyser)Yashdeep Sharma0% (1)