Das könnte Ihnen auch gefallen
- Army Weak LongDokument7 SeitenArmy Weak LongJoshua R. WalterNoch keine Bewertungen
- Strength Science 2012 by SullivanDokument64 SeitenStrength Science 2012 by SullivanAndrew ShirekNoch keine Bewertungen
- Misinflammation SullivanDokument24 SeitenMisinflammation SullivancomicreaderNoch keine Bewertungen
- Pulling Mechanism 2Dokument9 SeitenPulling Mechanism 2comicreaderNoch keine Bewertungen
- Learning Press RippetoeDokument8 SeitenLearning Press RippetoecomicreaderNoch keine Bewertungen
- 2011 Science SullivanDokument31 Seiten2011 Science SullivancomicreaderNoch keine Bewertungen
- SAS Survival GuideDokument193 SeitenSAS Survival Guidedaniel415198326Noch keine Bewertungen
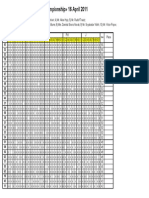
- 1/16 Fin World Latin Championship 16 April 2011: Cha Sa J PD RDokument16 Seiten1/16 Fin World Latin Championship 16 April 2011: Cha Sa J PD RcomicreaderNoch keine Bewertungen
- Stargate Magazine SamplerDokument23 SeitenStargate Magazine SamplerLeon BlažekovićNoch keine Bewertungen
- Theory of ConstraintsDokument12 SeitenTheory of ConstraintsVikas NandanwarNoch keine Bewertungen
- Passing the Guard Strategies for Streetfighting SituationsDokument5 SeitenPassing the Guard Strategies for Streetfighting SituationscomicreaderNoch keine Bewertungen
- Passing The Guard Ten Principals of GrapplingDokument2 SeitenPassing The Guard Ten Principals of GrapplingcomicreaderNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Mapeh WorksheetDokument16 SeitenMapeh WorksheetMelissa Rose Ignacio-GarciaNoch keine Bewertungen
- Isolasi Fungi EndofitDokument15 SeitenIsolasi Fungi EndofitZayyin WardiahNoch keine Bewertungen
- CH 9-10 Ethical Demensions 6thDokument70 SeitenCH 9-10 Ethical Demensions 6thSteven ChikNoch keine Bewertungen
- Unani IntroductionDokument37 SeitenUnani Introductionhabib_VNoch keine Bewertungen
- Normal LabourDokument55 SeitenNormal LabourSalshabilNoch keine Bewertungen
- EbolaDokument4 SeitenEbolaapi-271224704Noch keine Bewertungen
- Health - Questions - Pdf-Igcse Biology WorksheetDokument22 SeitenHealth - Questions - Pdf-Igcse Biology WorksheetPrincess KimNoch keine Bewertungen
- Cystitis Treatment and CausesDokument13 SeitenCystitis Treatment and CausesVINCENT CHANDRA KUSUMANoch keine Bewertungen
- What To Expect After VaccinationsDokument2 SeitenWhat To Expect After Vaccinationsmunshimbwe munshimbweNoch keine Bewertungen
- Proiect de Absolvire: Şcoala Postliceală Sanitară Carol Davila" BucurestiDokument34 SeitenProiect de Absolvire: Şcoala Postliceală Sanitară Carol Davila" BucurestiValentin StefanNoch keine Bewertungen
- CASE PRESENTATION ON CAD-UNSTABLE ANGINA, HYPOKALEMIA, PARONYCHIADokument18 SeitenCASE PRESENTATION ON CAD-UNSTABLE ANGINA, HYPOKALEMIA, PARONYCHIASafoora RafeeqNoch keine Bewertungen
- DADHDokument69 SeitenDADHdrpnnreddyNoch keine Bewertungen
- Topic 3.9 To 3.14: Year: 12 Subject: Biology Unit: 3Dokument58 SeitenTopic 3.9 To 3.14: Year: 12 Subject: Biology Unit: 3reyaNoch keine Bewertungen
- Reading Tips TOEFLDokument34 SeitenReading Tips TOEFLFitri PuspasariNoch keine Bewertungen
- Radiologia en EndodonciaDokument12 SeitenRadiologia en EndodonciaBelez Jum JumNoch keine Bewertungen
- Renal Physiology TestsDokument27 SeitenRenal Physiology TestsHuzaifa KhanNoch keine Bewertungen
- ISONIAZIDDokument2 SeitenISONIAZIDPoet POet PoEtNoch keine Bewertungen
- Digital tools enhance clinical reasoningDokument7 SeitenDigital tools enhance clinical reasoningCésar LeónNoch keine Bewertungen
- 899 PDFDokument3 Seiten899 PDFManuel CarboNoch keine Bewertungen
- 02AdvancedThinkAhead3 Term2 TL2Dokument4 Seiten02AdvancedThinkAhead3 Term2 TL2natachaNoch keine Bewertungen
- CHAPTER 25 (Ergogenic Aids)Dokument44 SeitenCHAPTER 25 (Ergogenic Aids)Muhammad AidibNoch keine Bewertungen
- 2010 Nigeria Federal Budget ProposalDokument69 Seiten2010 Nigeria Federal Budget ProposalDon Pim PimNoch keine Bewertungen
- Cancer TreatmentDokument4 SeitenCancer TreatmentEpsilonxNoch keine Bewertungen
- Drug MenuDokument17 SeitenDrug MenukathlynmangasiNoch keine Bewertungen
- NCP BurnsDokument16 SeitenNCP BurnsfringsterNoch keine Bewertungen
- Anemia in ToddlersDokument14 SeitenAnemia in ToddlersEmily EresumaNoch keine Bewertungen
- Papilloma Skuamosa: Laporan Kasus Dan Tinjauan PustakaDokument4 SeitenPapilloma Skuamosa: Laporan Kasus Dan Tinjauan PustakarizkyayuarristaNoch keine Bewertungen
- Central Machinery Model 93212 Manual in EnglishDokument37 SeitenCentral Machinery Model 93212 Manual in EnglishNoel0% (1)
- FIQ - Proliferative Diabetic RetinopathyDokument35 SeitenFIQ - Proliferative Diabetic RetinopathyHikban FiqhiNoch keine Bewertungen
- What is GMO? The Complete GuideDokument7 SeitenWhat is GMO? The Complete GuidewerkaserkaNoch keine Bewertungen