Das könnte Ihnen auch gefallen
- ART - Spectrophotometric Method For Determining GA in ..Dokument4 SeitenART - Spectrophotometric Method For Determining GA in ..Azahara Linares100% (2)
- Evidence of Barriers To Evidence-Based Physiotherapy Practice in Northern AfricaDokument5 SeitenEvidence of Barriers To Evidence-Based Physiotherapy Practice in Northern AfricaDr. Krishna N. SharmaNoch keine Bewertungen
- Personal Development Lesson 2Dokument54 SeitenPersonal Development Lesson 2Ysay FranciscoNoch keine Bewertungen
- Literature Review CTW ReviewDokument12 SeitenLiterature Review CTW Reviewapi-556034404Noch keine Bewertungen
- 2 Ijmtst0810098Dokument6 Seiten2 Ijmtst0810098Vijay MuniNoch keine Bewertungen
- Mirror Therapy Enhances Motor Performance in The Paretic Upper Limb After Stroke: A Pilot Randomized Controlled TrialDokument6 SeitenMirror Therapy Enhances Motor Performance in The Paretic Upper Limb After Stroke: A Pilot Randomized Controlled TrialScientifica EducacionalNoch keine Bewertungen
- Effects of Short Term Water Immersion On Peripheral Reflex Excitability in Hemiplegic and Healthy Individuals: A Preliminary StudyDokument5 SeitenEffects of Short Term Water Immersion On Peripheral Reflex Excitability in Hemiplegic and Healthy Individuals: A Preliminary StudyJosevanlealNoch keine Bewertungen
- 9 - 5 - The Effect of Mirror Therapy On Balance Ability of Subacute Stroke Patients - Bella Syafitri PDFDokument6 Seiten9 - 5 - The Effect of Mirror Therapy On Balance Ability of Subacute Stroke Patients - Bella Syafitri PDFAkhyar FtNoch keine Bewertungen
- 165-Article Text-385-1-10-20190423Dokument7 Seiten165-Article Text-385-1-10-20190423Deva GeofahniNoch keine Bewertungen
- Noninvasive Activation of Cervical Spinal Networks After Severe ParalysisDokument24 SeitenNoninvasive Activation of Cervical Spinal Networks After Severe ParalysisAnonymous 0SjC1nVvNoch keine Bewertungen
- Background:: Kiran Prakash PappalaDokument7 SeitenBackground:: Kiran Prakash PappalaMunni KNoch keine Bewertungen
- Anusha Article IJIRMFDokument5 SeitenAnusha Article IJIRMFAnusha SampathNoch keine Bewertungen
- 10 1111@sms 13853Dokument17 Seiten10 1111@sms 13853Cintia BeatrizNoch keine Bewertungen
- Constraint Induced Manual TherapyDokument165 SeitenConstraint Induced Manual TherapyPrabhu Chinna Gounder100% (1)
- Comparison Between Effectiveness of Hand Arm Bimanual Intensive Training and Repetitive Facilitation Exercises On Upper Limb Functions in Post Stroke Hemiparetic PatientsDokument10 SeitenComparison Between Effectiveness of Hand Arm Bimanual Intensive Training and Repetitive Facilitation Exercises On Upper Limb Functions in Post Stroke Hemiparetic PatientsEditor IJTSRDNoch keine Bewertungen
- Publication 26Dokument8 SeitenPublication 26Siva Sankaran SNoch keine Bewertungen
- Comparison of Single-Session Dose Response Effects of Whole Body Vibration On Spasticity and Walking Speed in Persons With Spinal Cord InjuryDokument13 SeitenComparison of Single-Session Dose Response Effects of Whole Body Vibration On Spasticity and Walking Speed in Persons With Spinal Cord InjurylabsoneducationNoch keine Bewertungen
- Stroke and Neuroplasticity (1) ..Dokument3 SeitenStroke and Neuroplasticity (1) ..drprasantNoch keine Bewertungen
- The Impact of Whole Body Vibration Therapy On Spasticity and Disability of The Patients With Poststroke HemiplegiaDokument6 SeitenThe Impact of Whole Body Vibration Therapy On Spasticity and Disability of The Patients With Poststroke HemiplegialabsoneducationNoch keine Bewertungen
- Diabet Journal NeuropatiDokument7 SeitenDiabet Journal NeuropatiAkuww WinwinNoch keine Bewertungen
- Document ABHISHEK CHOUBAYDokument12 SeitenDocument ABHISHEK CHOUBAYRishika AhujaNoch keine Bewertungen
- Bahan Inc TranslateDokument8 SeitenBahan Inc TranslateDedi Irawandi Angela NursisNoch keine Bewertungen
- To Compare The Effectiveness of Constraint Induced Movement Therapy Versus Motor Relearning Programme To Improve Motor Function of Hemiplegic Upper Extremity After StrokeDokument5 SeitenTo Compare The Effectiveness of Constraint Induced Movement Therapy Versus Motor Relearning Programme To Improve Motor Function of Hemiplegic Upper Extremity After Strokerizk86Noch keine Bewertungen
- FESpaper 2015Dokument16 SeitenFESpaper 2015prettysia suvarlyNoch keine Bewertungen
- Stroke RehabilitationDokument10 SeitenStroke RehabilitationPethuel Pomaloy100% (1)
- Epilepsia SeriesDokument5 SeitenEpilepsia SeriesLuzz VelascoNoch keine Bewertungen
- Effects of Transcranial Direct Current Stimulat StudyDokument14 SeitenEffects of Transcranial Direct Current Stimulat Studydinto dNoch keine Bewertungen
- IRJP MirrorTherapyDokument6 SeitenIRJP MirrorTherapyRaka dewiNoch keine Bewertungen
- 31Dokument5 Seiten31Javier NoNoch keine Bewertungen
- Art 1Dokument10 SeitenArt 1ALEJANDRA GARZÓN CUELLAR.Noch keine Bewertungen
- Neurophysiological and Behavioural Adaptations To A Bilateral Training Intervention in Individuals Following StrokeDokument13 SeitenNeurophysiological and Behavioural Adaptations To A Bilateral Training Intervention in Individuals Following StrokeIcha Chaphedech hildantraNoch keine Bewertungen
- Compensation in Recovery of Upper Extremity Function After Stroke: The Copenhagen Stroke StudyDokument2 SeitenCompensation in Recovery of Upper Extremity Function After Stroke: The Copenhagen Stroke Studywsm20012k7Noch keine Bewertungen
- Journal ESWT Pada DewasaDokument7 SeitenJournal ESWT Pada DewasaPhilipusHendryHartonoNoch keine Bewertungen
- Upper Extremity Synergy Pattern: A Case Report Electromyographic Biofeedback To Dissociate AnDokument7 SeitenUpper Extremity Synergy Pattern: A Case Report Electromyographic Biofeedback To Dissociate AnJuliyya FranciscoNoch keine Bewertungen
- Home-Based - Electromyography-TrDokument10 SeitenHome-Based - Electromyography-Trjorgequintero927470Noch keine Bewertungen
- Influence of Myofacial Release and Stretching To Relieve Spasticity in Patients With Stroke - A Systematic ReviewDokument5 SeitenInfluence of Myofacial Release and Stretching To Relieve Spasticity in Patients With Stroke - A Systematic ReviewInternational Journal of Innovative Science and Research TechnologyNoch keine Bewertungen
- Stroke Rehab NIDokument11 SeitenStroke Rehab NIFruzsina ÜrmösNoch keine Bewertungen
- Motor Rehabilitation Following A Stroke-FinalDokument13 SeitenMotor Rehabilitation Following A Stroke-Finalapi-301429903Noch keine Bewertungen
- 79b6 PDFDokument5 Seiten79b6 PDFcnsatishNoch keine Bewertungen
- PGRB SynopsisDokument21 SeitenPGRB Synopsis2022824838.pasangNoch keine Bewertungen
- (31 36) V9N5PTDokument6 Seiten(31 36) V9N5PTASD2019Noch keine Bewertungen
- Clinical Study: Autologous Blood Injection and Wrist Immobilisation For Chronic Lateral EpicondylitisDokument6 SeitenClinical Study: Autologous Blood Injection and Wrist Immobilisation For Chronic Lateral EpicondylitistriptykhannaNoch keine Bewertungen
- Abstract BookDokument222 SeitenAbstract BookArkesh PatnaikNoch keine Bewertungen
- 01d3c134-0005-450f-9e4e-d814211ee29a (1)Dokument7 Seiten01d3c134-0005-450f-9e4e-d814211ee29a (1)Pinekeshi NikithaNoch keine Bewertungen
- Modified Rood's Approach and Ability of Independent Selfcare in Haemorrhagic Stroke Patients of Assam, IndiaDokument6 SeitenModified Rood's Approach and Ability of Independent Selfcare in Haemorrhagic Stroke Patients of Assam, Indianandhini raguNoch keine Bewertungen
- Asj 2020 0146Dokument6 SeitenAsj 2020 0146Mandeep JangraNoch keine Bewertungen
- Inter Fan ZhangDokument9 SeitenInter Fan ZhangrizkaNoch keine Bewertungen
- Functional Strength Training Versus Movement Performance Therapy For Upper Limb Motor Recovery Early After Stroke: A RCTDokument8 SeitenFunctional Strength Training Versus Movement Performance Therapy For Upper Limb Motor Recovery Early After Stroke: A RCTانجمن بدنسازی ایرانNoch keine Bewertungen
- 2 AgarwalDokument7 Seiten2 AgarwaleditorijmrhsNoch keine Bewertungen
- Synergistic Efficacy of Repetitive Peripheral MagneticDokument18 SeitenSynergistic Efficacy of Repetitive Peripheral Magneticadri ajaNoch keine Bewertungen
- Jurnal RomDokument8 SeitenJurnal RomPutri WulandariNoch keine Bewertungen
- To Compare The Effects of Maitland MobilizationDokument4 SeitenTo Compare The Effects of Maitland MobilizationravichandragoudaNoch keine Bewertungen
- Constraint Induced Movement TherapyDokument4 SeitenConstraint Induced Movement TherapyNikka VentorilloNoch keine Bewertungen
- A Comparative Study To Determine The Efficacy of Routine Physical Therapy Treatment With and Without Kaltenborn Mobilization On Pain and Shoulder Mobility in Frozen Shoulder PatientsDokument4 SeitenA Comparative Study To Determine The Efficacy of Routine Physical Therapy Treatment With and Without Kaltenborn Mobilization On Pain and Shoulder Mobility in Frozen Shoulder Patientsfi.afifah NurNoch keine Bewertungen
- 10 5923 J Stroke 20170501 01Dokument9 Seiten10 5923 J Stroke 20170501 01Cristian Florin CrasmaruNoch keine Bewertungen
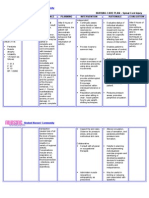
- Nursingcribcom Nursing Care Plan Spinal Cord InjuryDokument2 SeitenNursingcribcom Nursing Care Plan Spinal Cord InjuryJanine Erika Julom Brillantes100% (1)
- 1 Ijpotdec20171Dokument8 Seiten1 Ijpotdec20171TJPRC PublicationsNoch keine Bewertungen
- The Effect of Intradialytic Aerobic Exercise On Dialysis Efficacy in Hemodialysis Patients: A Randomized Controlled TrialDokument5 SeitenThe Effect of Intradialytic Aerobic Exercise On Dialysis Efficacy in Hemodialysis Patients: A Randomized Controlled TrialFitriatun NisaNoch keine Bewertungen
- The Effects of Taping Neuromuscular Compare To Physical Therapies Modalities in Patients With Adhesive Capsulitis of The ShoulderDokument8 SeitenThe Effects of Taping Neuromuscular Compare To Physical Therapies Modalities in Patients With Adhesive Capsulitis of The ShouldersilviaNoch keine Bewertungen
- Clinical StudyDokument8 SeitenClinical Studylilis pratiwiNoch keine Bewertungen
- IOT Based Wireless Monitoring Stroke Patient With Partial Paralysis AssistanceDokument7 SeitenIOT Based Wireless Monitoring Stroke Patient With Partial Paralysis AssistanceAzmi AbdulbaqiNoch keine Bewertungen
- Summary of Peter G. Levine's Stronger After Stroke, Third EditionVon EverandSummary of Peter G. Levine's Stronger After Stroke, Third EditionNoch keine Bewertungen
- A Simple Guide to Post-stroke Recovery, Diagnosis, Treatment and Related ConditionsVon EverandA Simple Guide to Post-stroke Recovery, Diagnosis, Treatment and Related ConditionsNoch keine Bewertungen
- Respiratory Physiotherapy in Triple Vessel Disease With Post Coronary Artery Bypass Grafting Surgery (CABG) SRJI Vol 2 Issue 3 Year 2013Dokument4 SeitenRespiratory Physiotherapy in Triple Vessel Disease With Post Coronary Artery Bypass Grafting Surgery (CABG) SRJI Vol 2 Issue 3 Year 2013Dr. Krishna N. SharmaNoch keine Bewertungen
- Scientific Research Journal of India ScReJI Volume 7 Issue 2 Year 2023Dokument53 SeitenScientific Research Journal of India ScReJI Volume 7 Issue 2 Year 2023Dr. Krishna N. SharmaNoch keine Bewertungen
- Scientific Research Journal of India SRJI Complete Vol-1 2012 All IssuesDokument233 SeitenScientific Research Journal of India SRJI Complete Vol-1 2012 All IssuesDr. Krishna N. SharmaNoch keine Bewertungen
- Scientific Research Journal of India SRJI Complete Vol-4 2015 All IssuesDokument53 SeitenScientific Research Journal of India SRJI Complete Vol-4 2015 All IssuesDr. Krishna N. SharmaNoch keine Bewertungen
- Scientific Research Journal of India SRJI Complete Vol-5 2016-2021 All IssuesDokument30 SeitenScientific Research Journal of India SRJI Complete Vol-5 2016-2021 All IssuesDr. Krishna N. SharmaNoch keine Bewertungen
- Ito Test: Does Height of The Pad Affect Back Muscle Endurance?Dokument7 SeitenIto Test: Does Height of The Pad Affect Back Muscle Endurance?Dr. Krishna N. SharmaNoch keine Bewertungen
- Mayank Pushkar. Congenital Talipes Equinovarus (CTEV) SRJI Vol - 2, Issue - 1, Year - 2013Dokument7 SeitenMayank Pushkar. Congenital Talipes Equinovarus (CTEV) SRJI Vol - 2, Issue - 1, Year - 2013Dr. Krishna N. SharmaNoch keine Bewertungen
- Physiotherapy Intervention in Management of Dizziness: Shahanawaz SDDokument11 SeitenPhysiotherapy Intervention in Management of Dizziness: Shahanawaz SDDr. Krishna N. SharmaNoch keine Bewertungen
- Pranjal Parmar. Comparison of The Effect of Isometric Exercise of Upper Limb On Vitals Between Young Males and FemalesDokument13 SeitenPranjal Parmar. Comparison of The Effect of Isometric Exercise of Upper Limb On Vitals Between Young Males and FemalesDr. Krishna N. SharmaNoch keine Bewertungen
- Occupational Therapy Marketing Indian Prospective SRJI Vol 2 Issue 3 Year 2013Dokument8 SeitenOccupational Therapy Marketing Indian Prospective SRJI Vol 2 Issue 3 Year 2013Dr. Krishna N. SharmaNoch keine Bewertungen
- Effectiveness of Core Strengthening Exercises To Reduce Incidence of Side Strain Injury in Medium Pace BowlersDokument12 SeitenEffectiveness of Core Strengthening Exercises To Reduce Incidence of Side Strain Injury in Medium Pace BowlersDr. Krishna N. SharmaNoch keine Bewertungen
- Parmar Sanjay T., Nayana A. Khobre. Growth in Cerebral Palsy Children Between 3-13 Years in Urban Dharwad, IndiaDokument7 SeitenParmar Sanjay T., Nayana A. Khobre. Growth in Cerebral Palsy Children Between 3-13 Years in Urban Dharwad, IndiaDr. Krishna N. SharmaNoch keine Bewertungen
- Impact of Ageing On Depression and Activities of Daily Livings in Normal Elderly Subjects Living in Old Age Homes and Communities of Kanpur, U.PDokument8 SeitenImpact of Ageing On Depression and Activities of Daily Livings in Normal Elderly Subjects Living in Old Age Homes and Communities of Kanpur, U.PDr. Krishna N. SharmaNoch keine Bewertungen
- Ethical Challenges For Occupational Therapist in India To Use Social MediaDokument6 SeitenEthical Challenges For Occupational Therapist in India To Use Social MediaDr. Krishna N. SharmaNoch keine Bewertungen
- Exploring The Roots of ElectrotherapyDokument4 SeitenExploring The Roots of ElectrotherapyDr. Krishna N. SharmaNoch keine Bewertungen
- Network Border Patrol Eradicates The Over Loading of Data Packets and Prevents Congestion Collapse Thereby Promoting Fairness Over TCP Protocol in LAN WAN SRJI Vol-1 Issue-1 Year-2013Dokument10 SeitenNetwork Border Patrol Eradicates The Over Loading of Data Packets and Prevents Congestion Collapse Thereby Promoting Fairness Over TCP Protocol in LAN WAN SRJI Vol-1 Issue-1 Year-2013Dr. Krishna N. SharmaNoch keine Bewertungen
- Evidence of Barriers To Evidence-Based Physiotherapy Practice in Nothern AfricaDokument7 SeitenEvidence of Barriers To Evidence-Based Physiotherapy Practice in Nothern AfricaDr. Krishna N. SharmaNoch keine Bewertungen
- Efficacy of 3D Gliding On Pain in Patients With Knee Osteoarthritis A Randomized Controlled Pilot StudyDokument5 SeitenEfficacy of 3D Gliding On Pain in Patients With Knee Osteoarthritis A Randomized Controlled Pilot StudyDr. Krishna N. SharmaNoch keine Bewertungen
- Efficacy of Retrowalking in Patients With Chronic Knee Osteoarthritis: A Single Group Experimental Pilot StudyDokument9 SeitenEfficacy of Retrowalking in Patients With Chronic Knee Osteoarthritis: A Single Group Experimental Pilot StudyDr. Krishna N. SharmaNoch keine Bewertungen
- Effects of Bimanual Functional Practice Training On Functional Performance of Upper Extremity in Chronic Stroke SRJI Vol 2 Issue 3 Year 2013Dokument10 SeitenEffects of Bimanual Functional Practice Training On Functional Performance of Upper Extremity in Chronic Stroke SRJI Vol 2 Issue 3 Year 2013Dr. Krishna N. SharmaNoch keine Bewertungen
- Effectiveness of Neuromotor Task Training Combined With Kinaesthetic Training in Children With Developmental Co - Ordination Disorder - A Randomised Trial SRJI Vol-1 Issue-1 Year-2013Dokument15 SeitenEffectiveness of Neuromotor Task Training Combined With Kinaesthetic Training in Children With Developmental Co - Ordination Disorder - A Randomised Trial SRJI Vol-1 Issue-1 Year-2013Dr. Krishna N. SharmaNoch keine Bewertungen
- Effectiveness of Supervised Graded Repetitive Arm Supplementary Program On Arm Function in Subjects With StrokeDokument10 SeitenEffectiveness of Supervised Graded Repetitive Arm Supplementary Program On Arm Function in Subjects With StrokeDr. Krishna N. SharmaNoch keine Bewertungen
- Full Journal SRJI Volume-1 Issue-3 Year-2012 Scientific Research Journal of IndiaDokument81 SeitenFull Journal SRJI Volume-1 Issue-3 Year-2012 Scientific Research Journal of IndiaDr. Krishna N. SharmaNoch keine Bewertungen
- Effects of Task Related Sitting Training On Balance in Hemiplegic Patients. Dr. Vivek H. Ramanandi Srji Vol 1 Issue 4 Year 2013Dokument9 SeitenEffects of Task Related Sitting Training On Balance in Hemiplegic Patients. Dr. Vivek H. Ramanandi Srji Vol 1 Issue 4 Year 2013Dr. Krishna N. SharmaNoch keine Bewertungen
- Editorial Srji Vol 3 Issue 2 Year 2014Dokument1 SeiteEditorial Srji Vol 3 Issue 2 Year 2014Dr. Krishna N. SharmaNoch keine Bewertungen
- Effectiveness of Conventional Physical Therapy & C.P.M Unit For Functional Rehabilitation After Total Knee ArthroplastyDokument21 SeitenEffectiveness of Conventional Physical Therapy & C.P.M Unit For Functional Rehabilitation After Total Knee ArthroplastyDr. Krishna N. SharmaNoch keine Bewertungen
- EditorialDokument1 SeiteEditorialDr. Krishna N. SharmaNoch keine Bewertungen
- Effect of Core Stabilization Training On Endurance of Trunk Extensor and Functional Capacity in Subjects With Mechanical Low Back PainDokument8 SeitenEffect of Core Stabilization Training On Endurance of Trunk Extensor and Functional Capacity in Subjects With Mechanical Low Back PainDr. Krishna N. SharmaNoch keine Bewertungen
- Editorial Vol 1 Issue 2. (Scientific Research Journal of India)Dokument2 SeitenEditorial Vol 1 Issue 2. (Scientific Research Journal of India)Dr. Krishna N. SharmaNoch keine Bewertungen
- Guideline For Prevention of Surgical Wound InfectionsDokument14 SeitenGuideline For Prevention of Surgical Wound InfectionsosaqerNoch keine Bewertungen
- Killing of Kangaroos For Meat and SkinDokument34 SeitenKilling of Kangaroos For Meat and SkinVegan FutureNoch keine Bewertungen
- Understandings, Applications and Skills (This Is What You Maybe Assessed On)Dokument10 SeitenUnderstandings, Applications and Skills (This Is What You Maybe Assessed On)beaNoch keine Bewertungen
- Preliminary Experiment: Visual Observation and InterpretationDokument3 SeitenPreliminary Experiment: Visual Observation and InterpretationRuchie Ann Pono BaraquilNoch keine Bewertungen
- 1 s2.0 S222541102200030X MainDokument11 Seiten1 s2.0 S222541102200030X Mainaman babuNoch keine Bewertungen
- Email To Professor SampleDokument6 SeitenEmail To Professor SamplesimplecobraNoch keine Bewertungen
- 300 One Word Substitutions Asked in SSC IBPS UPSC ExamDokument12 Seiten300 One Word Substitutions Asked in SSC IBPS UPSC ExamRashid AliNoch keine Bewertungen
- Chauhan2017mulberry SericultureDokument67 SeitenChauhan2017mulberry SericultureNarasimha Murthy S VNoch keine Bewertungen
- FTS - 11 (Code-A) - 24-04-2020 PDFDokument16 SeitenFTS - 11 (Code-A) - 24-04-2020 PDFkavyareddyNoch keine Bewertungen
- Tule Elk in Point ReyesDokument4 SeitenTule Elk in Point ReyesPointReyesNoch keine Bewertungen
- Hamsters - A General DescriptionDokument5 SeitenHamsters - A General Descriptiondulce crissNoch keine Bewertungen
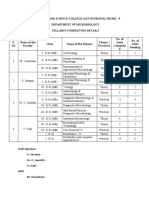
- Syllabus CompletionDokument1 SeiteSyllabus CompletiongopimicroNoch keine Bewertungen
- 3-MS Examples PDFDokument59 Seiten3-MS Examples PDFlexuanminhk54lochoaNoch keine Bewertungen
- Qualitative and QuantitativeDokument2 SeitenQualitative and Quantitativetimmierivera100% (1)
- Why Do Giraffes Have Long Necks?Dokument22 SeitenWhy Do Giraffes Have Long Necks?johnosborneNoch keine Bewertungen
- Contoh Rencana Studi LPDPDokument3 SeitenContoh Rencana Studi LPDPZahid ZainNoch keine Bewertungen
- Cell Cycle BrainstormingDokument3 SeitenCell Cycle BrainstormingKimberley MendozaNoch keine Bewertungen
- MHE RDG Wonders LVRDR G3 ELL U4W3 18Dokument24 SeitenMHE RDG Wonders LVRDR G3 ELL U4W3 18Kenneth N AngelineNoch keine Bewertungen
- MSDS Ecaro-25Dokument10 SeitenMSDS Ecaro-25ValenteNoch keine Bewertungen
- Jane Goodall BiographyDokument2 SeitenJane Goodall BiographyOjas JangalNoch keine Bewertungen
- Selina Solutions For Class 9 Biology Chapter 2 Cell The Unit of LifeDokument15 SeitenSelina Solutions For Class 9 Biology Chapter 2 Cell The Unit of LifePrashun PriyadarshiNoch keine Bewertungen
- ALB2Dokument4 SeitenALB2Jonalyn SalandoNoch keine Bewertungen
- Science Paper 7 - SolvedDokument10 SeitenScience Paper 7 - SolvedRavi KumarNoch keine Bewertungen
- A Substitution Mutation in The Myosin Binding Protein C Gene in Ragdoll Hypertrophic CardiomyopathyDokument4 SeitenA Substitution Mutation in The Myosin Binding Protein C Gene in Ragdoll Hypertrophic CardiomyopathyRoy SzeNoch keine Bewertungen
- CV Christopher Lean Jan 2024 Without ReferencesDokument5 SeitenCV Christopher Lean Jan 2024 Without Referencesapi-399765628Noch keine Bewertungen
- Jellyfish Research PaperDokument6 SeitenJellyfish Research Papergzrvpcvnd100% (1)
- 0 AlignMeDokument6 Seiten0 AlignMeCRISTIAN GABRIEL ZAMBRANO VEGANoch keine Bewertungen
- Can The Unconscious Mind Be Persuaded? An Overview With Marketing ImplicationsDokument9 SeitenCan The Unconscious Mind Be Persuaded? An Overview With Marketing ImplicationsAhmed El-ShafeiNoch keine Bewertungen