Das könnte Ihnen auch gefallen
- The Code Stroke Handbook: Approach to the Acute Stroke PatientVon EverandThe Code Stroke Handbook: Approach to the Acute Stroke PatientNoch keine Bewertungen
- Textbook of Urgent Care Management: Chapter 39, Ensuring Patient SafetyVon EverandTextbook of Urgent Care Management: Chapter 39, Ensuring Patient SafetyNoch keine Bewertungen
- RCH DEM Head Injury GuidelinesDokument4 SeitenRCH DEM Head Injury GuidelinesJerry LeeNoch keine Bewertungen
- Assessment and Diagnostic FindingsDokument7 SeitenAssessment and Diagnostic FindingsAlmustapha Babangida DanganiNoch keine Bewertungen
- Thesis On Birth AsphyxiaDokument4 SeitenThesis On Birth Asphyxiaimmkhuwhd100% (3)
- Cec Post Fall Assess and Man June 2013Dokument3 SeitenCec Post Fall Assess and Man June 2013Vicente TurasNoch keine Bewertungen
- Pediatric Trauma Care EssentialsDokument39 SeitenPediatric Trauma Care Essentialspuja argaNoch keine Bewertungen
- Trauma in Children: Initial Assessment and ManagementDokument39 SeitenTrauma in Children: Initial Assessment and ManagementDrTushar GoswamiNoch keine Bewertungen
- Ebook Cardiovaskuler Disease StrokeDokument9 SeitenEbook Cardiovaskuler Disease StrokearisNoch keine Bewertungen
- NewbornEmergenices2006 PDFDokument16 SeitenNewbornEmergenices2006 PDFRana SalemNoch keine Bewertungen
- Updatesinthegeneralapproach Topediatricheadtraumaand ConcussionDokument16 SeitenUpdatesinthegeneralapproach Topediatricheadtraumaand ConcussionDavid MirandaNoch keine Bewertungen
- Head Injury Management of PediatricDokument22 SeitenHead Injury Management of PediatricIrma KusumaNoch keine Bewertungen
- Care of Child with Head Injury and HydrocephalusDokument34 SeitenCare of Child with Head Injury and HydrocephalusSHAFIQNoch keine Bewertungen
- Research: CATCH: A Clinical Decision Rule For The Use of Computed Tomography in Children With Minor Head InjuryDokument8 SeitenResearch: CATCH: A Clinical Decision Rule For The Use of Computed Tomography in Children With Minor Head InjuryCarlos Martin Yafac RiscoNoch keine Bewertungen
- 100 Case Studies in Pathophysiology-532hlm (Warna Hanya Cover)Dokument11 Seiten100 Case Studies in Pathophysiology-532hlm (Warna Hanya Cover)Haymanot AnimutNoch keine Bewertungen
- Seizures+in+Children_Paed_v4_1Dokument10 SeitenSeizures+in+Children_Paed_v4_1mahmudajannatul.7Noch keine Bewertungen
- Escherichia Coli Streptococcus Group B Haemophilus Influenzae Streptococcus Pneumoniae Neisseria Meningitides Staphylococcus AureusDokument4 SeitenEscherichia Coli Streptococcus Group B Haemophilus Influenzae Streptococcus Pneumoniae Neisseria Meningitides Staphylococcus AureusBrent NicholsNoch keine Bewertungen
- Screenshot 2022-12-19 at 7.25.46 AMDokument45 SeitenScreenshot 2022-12-19 at 7.25.46 AMFhaiiee SalapudinNoch keine Bewertungen
- Valoración PreanestesicaDokument5 SeitenValoración PreanestesicaSebastian Hdez BolañosNoch keine Bewertungen
- Head Injury: Triage, Assessment, Investigation and Early Management of Head Injury in Infants, Children and AdultsDokument231 SeitenHead Injury: Triage, Assessment, Investigation and Early Management of Head Injury in Infants, Children and Adultsakunkeren2023Noch keine Bewertungen
- Epilepsy+pregnancy+management Clinical+Guideline Final Dec14Dokument14 SeitenEpilepsy+pregnancy+management Clinical+Guideline Final Dec14Marizka Putri AftriaNoch keine Bewertungen
- The Pediatric Physical Examination - HEENT - UpToDateDokument87 SeitenThe Pediatric Physical Examination - HEENT - UpToDateEmily LinharesNoch keine Bewertungen
- Research Paper On Shaken Baby SyndromeDokument8 SeitenResearch Paper On Shaken Baby Syndromefys4gjmk100% (1)
- Approach To HeadacheDokument61 SeitenApproach To Headachesabahat.husainNoch keine Bewertungen
- Anzcor Guideline 9 2 12 Seriously Ill Person April 2021Dokument5 SeitenAnzcor Guideline 9 2 12 Seriously Ill Person April 2021hernandez2812Noch keine Bewertungen
- PECARN Algorithms For Minor Head TraumaDokument11 SeitenPECARN Algorithms For Minor Head Traumaedgarjavier65Noch keine Bewertungen
- Anciano - Niño en Urg Emerg Med Clin Ona Ago 17 PDFDokument15 SeitenAnciano - Niño en Urg Emerg Med Clin Ona Ago 17 PDFLuis ParraNoch keine Bewertungen
- Pediatric Trauma: Presented By: Erwin MaulanaDokument39 SeitenPediatric Trauma: Presented By: Erwin Maulanaadliah zahiraNoch keine Bewertungen
- Epilepsies in Children, Young People, and Adults: Summary of Updated NICE GuidanceDokument13 SeitenEpilepsies in Children, Young People, and Adults: Summary of Updated NICE GuidanceANDREWNoch keine Bewertungen
- Material paraDokument89 SeitenMaterial pararoberto gomesNoch keine Bewertungen
- Neurologic Emergencies 2 MergedDokument71 SeitenNeurologic Emergencies 2 MergedDanica FrancoNoch keine Bewertungen
- Cerebral Palsy Etiology, Evaluation, and Management of The Most Common Cause For Pediatric DisabilityDokument14 SeitenCerebral Palsy Etiology, Evaluation, and Management of The Most Common Cause For Pediatric DisabilityDavid ParraNoch keine Bewertungen
- The Kids Are Alright Pediatric Trauma PearlsDokument21 SeitenThe Kids Are Alright Pediatric Trauma PearlsDaniel Torres CutivaNoch keine Bewertungen
- Neonatal Encephalopathy GuidelineDokument41 SeitenNeonatal Encephalopathy GuidelineMadelein Claros Euscate0% (1)
- 2022 - McIntyre - Global Prevalence CPDokument13 Seiten2022 - McIntyre - Global Prevalence CPFriendlymeNoch keine Bewertungen
- Surgical Management of Otitis Media With Effusion in ChildrenDokument22 SeitenSurgical Management of Otitis Media With Effusion in ChildrenGerry Raymond JovioloNoch keine Bewertungen
- Head InjuryDokument18 SeitenHead InjuryVasantharaja ManipillaiNoch keine Bewertungen
- To Be ConDokument53 SeitenTo Be ConLiza AingelicaNoch keine Bewertungen
- Introduction to Cerebral Palsy: Causes, Symptoms, Diagnosis and TreatmentDokument23 SeitenIntroduction to Cerebral Palsy: Causes, Symptoms, Diagnosis and TreatmentVenkata Nagaraj Mummadisetty100% (1)
- MM Guidelines 2010Dokument5 SeitenMM Guidelines 2010Arimbi DrestiNoch keine Bewertungen
- Baby Shaking Syndrome PresentationDokument4 SeitenBaby Shaking Syndrome PresentationAnastasia BorsNoch keine Bewertungen
- Medical Emergency in Paediatric Dental ClinicDokument75 SeitenMedical Emergency in Paediatric Dental ClinicAkshay Sreeraman KecheryNoch keine Bewertungen
- Shaken Baby Syndrome A Review of 20 CasesDokument4 SeitenShaken Baby Syndrome A Review of 20 Casestamis1982Noch keine Bewertungen
- 3.the Efficient Dizziness History and ExamDokument12 Seiten3.the Efficient Dizziness History and ExamCribea AdmNoch keine Bewertungen
- Case 9: 2-Week-Old With Lethargy - CrimsonDokument7 SeitenCase 9: 2-Week-Old With Lethargy - Crimsonalwaysbeclosing52Noch keine Bewertungen
- Head Injury NICE GuidelineDokument54 SeitenHead Injury NICE GuidelineIrina Garlea-RobuNoch keine Bewertungen
- An Introduction To Tuberous Sclerosis ComplexDokument20 SeitenAn Introduction To Tuberous Sclerosis ComplexArif KurniadiNoch keine Bewertungen
- NSG124 - 16 Alteration in Nervous SystemDokument11 SeitenNSG124 - 16 Alteration in Nervous Systemlaurie.charlynjaneNoch keine Bewertungen
- Guidelines On Neonatal ExaminationDokument9 SeitenGuidelines On Neonatal ExaminationShitanjni WatiNoch keine Bewertungen
- Manejo de Traumatismo Mayor en PediatriaDokument8 SeitenManejo de Traumatismo Mayor en Pediatriasucy asto fabianNoch keine Bewertungen
- Amb AnesthesiaDokument11 SeitenAmb AnesthesiaPooh AngelNoch keine Bewertungen
- SCIWORA-Spinal Cord Injury Without Radiological Abnormality: Veena Kalra, Sheffali Gulati, Mahesh Kamate and Ajay GargDokument3 SeitenSCIWORA-Spinal Cord Injury Without Radiological Abnormality: Veena Kalra, Sheffali Gulati, Mahesh Kamate and Ajay GargnsatriotomoNoch keine Bewertungen
- TbiguidelineDokument8 SeitenTbiguidelinearifbudipraNoch keine Bewertungen
- Sumber 9Dokument18 SeitenSumber 9Ali Laksana SuryaNoch keine Bewertungen
- NeuroSystem Chapter 47Dokument71 SeitenNeuroSystem Chapter 47Cecil MonteroNoch keine Bewertungen
- WFSA Craniopharyngioma Resection PDFDokument5 SeitenWFSA Craniopharyngioma Resection PDFpitriaNoch keine Bewertungen
- Cerebral Palsy Prep CardDokument4 SeitenCerebral Palsy Prep CardBenNoch keine Bewertungen
- SAQs PaediatricsDokument43 SeitenSAQs Paediatricss336336anl100% (1)
- Pregnancy and Brain TumourDokument10 SeitenPregnancy and Brain TumourDuddy Ari HardiantoNoch keine Bewertungen
- Case study on cerebral palsy managementDokument15 SeitenCase study on cerebral palsy managementjudii01Noch keine Bewertungen
- Purposive Communication: Republic of The Philippines Province of Ilocos Sur Ilocos Sur Community College Vigan CityDokument7 SeitenPurposive Communication: Republic of The Philippines Province of Ilocos Sur Ilocos Sur Community College Vigan CityLes GasparNoch keine Bewertungen
- 40 Business Book SummariesDokument196 Seiten40 Business Book SummariesAnshuman SrivastavaNoch keine Bewertungen
- Article On Globalization in Nepal and Its OppotunitiesDokument6 SeitenArticle On Globalization in Nepal and Its OppotunitiesReema KhatryNoch keine Bewertungen
- Business PlanDokument8 SeitenBusiness PlanyounggirldavidNoch keine Bewertungen
- Deviz 12 KW Cu Invertor de 15 KWDokument2 SeitenDeviz 12 KW Cu Invertor de 15 KWcontscribdNoch keine Bewertungen
- The dangers of electrostatic phenomenaDokument14 SeitenThe dangers of electrostatic phenomenaYaminNoch keine Bewertungen
- [Advances in Neurosurgery 2] O. Stochdorph (Auth.), W. Klug, M. Brock, M. Klinger, O. Spoerri (Eds.) - Meningiomas Diagnostic and Therapeutic Problems Multiple Sclerosis Misdiagnosis Forensic Problems in NeurosurgDokument461 Seiten[Advances in Neurosurgery 2] O. Stochdorph (Auth.), W. Klug, M. Brock, M. Klinger, O. Spoerri (Eds.) - Meningiomas Diagnostic and Therapeutic Problems Multiple Sclerosis Misdiagnosis Forensic Problems in Neurosurgbayu_gendeng666Noch keine Bewertungen
- 2009 - Mazars Insight Ifrs 5 enDokument36 Seiten2009 - Mazars Insight Ifrs 5 enSahar FekihNoch keine Bewertungen
- Batch Op LOPA WorksheetDokument35 SeitenBatch Op LOPA WorksheetShruti JoshiNoch keine Bewertungen
- Oxford Classical Dictionary AbbreviationsDokument9 SeitenOxford Classical Dictionary AbbreviationsScotch_Nights_Order0% (2)
- Pilani MTech SS PDFDokument12 SeitenPilani MTech SS PDFonline accountNoch keine Bewertungen
- VE With CLE 10-Module 22-4th Quarter - CASTRODokument5 SeitenVE With CLE 10-Module 22-4th Quarter - CASTRORojan ClarkNoch keine Bewertungen
- Prueba Final Inglres Robert PalaciosDokument2 SeitenPrueba Final Inglres Robert PalaciosCarlos GuerreroNoch keine Bewertungen
- Business Research Study Material - Calicut UniversityDokument50 SeitenBusiness Research Study Material - Calicut UniversityDr Linda Mary SimonNoch keine Bewertungen
- Internal Control QuestionnaireDokument19 SeitenInternal Control QuestionnaireIchsanNoch keine Bewertungen
- FS 3 Technology in The Learning EnvironmentDokument24 SeitenFS 3 Technology in The Learning EnvironmentJayson Gelera CabrigasNoch keine Bewertungen
- VRF, MPLS and MP-BGP FundamentalsDokument55 SeitenVRF, MPLS and MP-BGP FundamentalsIVAN TANEV100% (2)
- Stock TakeDokument14 SeitenStock Takesafare2222Noch keine Bewertungen
- Energy Savings White PaperDokument14 SeitenEnergy Savings White PapersajuhereNoch keine Bewertungen
- Soal Bing XiDokument9 SeitenSoal Bing XiRhya GomangNoch keine Bewertungen
- TB170LSDokument4 SeitenTB170LSDary ArroyoNoch keine Bewertungen
- Anatomija Za Umetnike PDFDokument4 SeitenAnatomija Za Umetnike PDFДанило ВујачићNoch keine Bewertungen
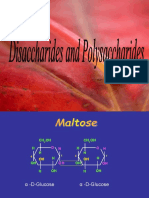
- Disaccharides and PolysaccharidesDokument17 SeitenDisaccharides and PolysaccharidesAarthi shreeNoch keine Bewertungen
- ROM Laboratory v1.00Dokument548 SeitenROM Laboratory v1.00Carlos Reaper Jaque OlivaresNoch keine Bewertungen
- Levitator Ino - InoDokument2 SeitenLevitator Ino - InoSUBHANKAR BAGNoch keine Bewertungen
- Developmental AssessmentDokument15 SeitenDevelopmental AssessmentShailesh MehtaNoch keine Bewertungen
- Sample Action Research in MathDokument12 SeitenSample Action Research in MathKresta BenignoNoch keine Bewertungen
- The Dilemma of Recognition Experienced Reality of Ethnicised Politics in Rwanda and BurundiDokument192 SeitenThe Dilemma of Recognition Experienced Reality of Ethnicised Politics in Rwanda and BurundiShenandoa LeãoNoch keine Bewertungen
- "Leadership Does Not Always Wear The Harness of Compromise." - Woodrow WilsonDokument3 Seiten"Leadership Does Not Always Wear The Harness of Compromise." - Woodrow WilsonAmbreen Zaineb/Lecturer BKR/Economics and BANoch keine Bewertungen

































































![[Advances in Neurosurgery 2] O. Stochdorph (Auth.), W. Klug, M. Brock, M. Klinger, O. Spoerri (Eds.) - Meningiomas Diagnostic and Therapeutic Problems Multiple Sclerosis Misdiagnosis Forensic Problems in Neurosurg](https://imgv2-2-f.scribdassets.com/img/document/375359245/149x198/fae4c10859/1522685798?v=1)