Das könnte Ihnen auch gefallen
- IM On Call (LANGE On Call) PDFDokument738 SeitenIM On Call (LANGE On Call) PDFindia2puppy100% (8)
- AKP Paper 2 PDFDokument54 SeitenAKP Paper 2 PDFMostafa Mahmoud Elsebey100% (2)
- Caso Clinico Electivas 3Dokument9 SeitenCaso Clinico Electivas 3MARIANGEL LAFONTNoch keine Bewertungen
- Dubin ECG Reference SheetsDokument13 SeitenDubin ECG Reference SheetsEllie100% (1)
- Summary of ECG AbnormalitiesDokument8 SeitenSummary of ECG AbnormalitiesChristine Nancy NgNoch keine Bewertungen
- Case Presentation Station 3B Drug Study TramadolDokument3 SeitenCase Presentation Station 3B Drug Study TramadolhahahahaaaaaaaNoch keine Bewertungen
- Physical Assessment and GordonsDokument14 SeitenPhysical Assessment and GordonsRubelyn Joy LazarteNoch keine Bewertungen
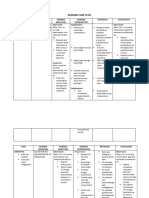
- Nursing Care Plan: Interaction Immediate Cause Goal: Effectivenes SDokument6 SeitenNursing Care Plan: Interaction Immediate Cause Goal: Effectivenes SCatherine Kaye Marquez RoxasNoch keine Bewertungen
- NCP EsrdDokument2 SeitenNCP EsrdAziil LiizaNoch keine Bewertungen
- Study Notes Emergency MedicineDokument12 SeitenStudy Notes Emergency MedicineMedShare57% (7)
- Management of Patients With Dysrhythmias and Conduction Problems Dr. SydioncoDokument15 SeitenManagement of Patients With Dysrhythmias and Conduction Problems Dr. SydioncoRoyce Vincent Tizon100% (1)
- Pemasangan Dan Interpretasi EKGDokument117 SeitenPemasangan Dan Interpretasi EKGaulianadanisya100% (2)
- Handbook of AnesthesiologyDokument176 SeitenHandbook of AnesthesiologyarmelzahfauziNoch keine Bewertungen
- ACLS For TachycardiaDokument31 SeitenACLS For TachycardiaTausif HaqueNoch keine Bewertungen
- 1 The General SurveyDokument6 Seiten1 The General SurveyLouisaRedobleNoch keine Bewertungen
- Gordons Threatened AbortionDokument2 SeitenGordons Threatened AbortionRobel_Saoi_2309Noch keine Bewertungen
- Gordons2 CHECK Nyo Nlng..Dokument7 SeitenGordons2 CHECK Nyo Nlng..ackela15Noch keine Bewertungen
- Gordon'S Health Pattern: Submitted To: Marjorie L. Apao, RNDokument6 SeitenGordon'S Health Pattern: Submitted To: Marjorie L. Apao, RNEnrique LuNoch keine Bewertungen
- Gi-Rle - NCP For Deficient Fluid VolumeDokument2 SeitenGi-Rle - NCP For Deficient Fluid VolumeEvangeline Villa de Gracia100% (1)
- Learning Feedback Diary and FamilyDokument2 SeitenLearning Feedback Diary and FamilyKenny GustavoNoch keine Bewertungen
- Which It Is A Process Whereby Pancreatic Enzymes Destroy Its Own Tissue Leading ToDokument8 SeitenWhich It Is A Process Whereby Pancreatic Enzymes Destroy Its Own Tissue Leading ToAriane-Gay Cristobal DuranNoch keine Bewertungen
- Sapna NCPDokument22 SeitenSapna NCPgill priyaNoch keine Bewertungen
- Nursing Health History 3rd YrDokument3 SeitenNursing Health History 3rd Yrshin_2173100% (1)
- Mr. Jones Case StudyDokument4 SeitenMr. Jones Case StudyDiane JaravataNoch keine Bewertungen
- Propranolol 1 PresentationDokument17 SeitenPropranolol 1 Presentationapi-284092317100% (1)
- Health EducationDokument5 SeitenHealth EducationMichellin Lara VergaraNoch keine Bewertungen
- Manaois - SPIRITUALITY IN NURSING QUIZDokument3 SeitenManaois - SPIRITUALITY IN NURSING QUIZDan Dan Manaois100% (1)
- Gordon's Functional Health PatternsDokument2 SeitenGordon's Functional Health Patternsserarrist100% (2)
- Nursing Care PlanDokument10 SeitenNursing Care PlanMalou SanNoch keine Bewertungen
- Ethical BrochureDokument2 SeitenEthical Brochureapi-414703292100% (1)
- Appendicitis Case StudyDokument35 SeitenAppendicitis Case StudyWilliam Soneja CalapiniNoch keine Bewertungen
- AspirinDokument1 SeiteAspirinAmanda CoadNoch keine Bewertungen
- Nursing Health HistoryDokument1 SeiteNursing Health HistoryFirenze Fil100% (1)
- ASSESSMENTDokument2 SeitenASSESSMENTColeen PequitNoch keine Bewertungen
- NCP Otitis MediaDokument4 SeitenNCP Otitis MediaZillah KorrenNoch keine Bewertungen
- Case Analysis (Physical Assessment)Dokument4 SeitenCase Analysis (Physical Assessment)angelsykeNoch keine Bewertungen
- Examination of The Chest and LungsDokument5 SeitenExamination of The Chest and Lungsteena12aNoch keine Bewertungen
- NCP Episiotomy WoundDokument3 SeitenNCP Episiotomy WoundJP2001Noch keine Bewertungen
- Cues Nursing Diagnosis Scientific Reason Objective Nursing Intervention Rationale EvaluationDokument4 SeitenCues Nursing Diagnosis Scientific Reason Objective Nursing Intervention Rationale Evaluationjomsportg0% (1)
- Case Study Final PortraitDokument11 SeitenCase Study Final PortraitZhy CaluzaNoch keine Bewertungen
- Activity IntoleranceDokument2 SeitenActivity IntoleranceDiane AbanillaNoch keine Bewertungen
- Physical Assessment Appendix FinalDokument6 SeitenPhysical Assessment Appendix FinalLucelle ArellanoNoch keine Bewertungen
- Contents of FDAR ChartingDokument1 SeiteContents of FDAR Chartingkaycelyn jimenezNoch keine Bewertungen
- NCP - BronchopneumoniaDokument11 SeitenNCP - BronchopneumoniaMaria Ivy Mendoza100% (1)
- Gerontologic Health Promotion ActivityDokument3 SeitenGerontologic Health Promotion ActivityCorinne50% (2)
- Diabetes InsipidusDokument48 SeitenDiabetes InsipidusAhmed Fraz MamoonNoch keine Bewertungen
- Premenstrual Dysphoric DisorderDokument11 SeitenPremenstrual Dysphoric Disorderapi-3764215Noch keine Bewertungen
- Nursing Care Plan EportfolioDokument14 SeitenNursing Care Plan Eportfolioapi-279212367Noch keine Bewertungen
- IV. Physical Assessment Norms Actual Findings Interpretation and Analysis General Appearance Posture / GaitDokument9 SeitenIV. Physical Assessment Norms Actual Findings Interpretation and Analysis General Appearance Posture / GaitMarianne_Miraflo_154Noch keine Bewertungen
- NCP For Rapid Shallow BreathingDokument1 SeiteNCP For Rapid Shallow Breathingbamboo2dNoch keine Bewertungen
- Orientation On Community Health - Doh Programs & ServicesDokument11 SeitenOrientation On Community Health - Doh Programs & ServicesAudrey Beatrice ReyesNoch keine Bewertungen
- Nursing Care Plan 2Dokument6 SeitenNursing Care Plan 2ayanori_boyNoch keine Bewertungen
- Choledolithiasis Cs 103 1Dokument34 SeitenCholedolithiasis Cs 103 1Merlene Sarmiento SalungaNoch keine Bewertungen
- Nursing Care Plan: Subjective DataDokument4 SeitenNursing Care Plan: Subjective DataAbdallah AlasalNoch keine Bewertungen
- III. Physical Assessment FindingsDokument8 SeitenIII. Physical Assessment FindingsBilly Joe SincoNoch keine Bewertungen
- Cva Case StudyDokument31 SeitenCva Case StudyZoe AnnaNoch keine Bewertungen
- Patient Health HistoryDokument8 SeitenPatient Health HistoryRafi LabNoch keine Bewertungen
- Abdominal Case Study CompiledDokument392 SeitenAbdominal Case Study CompiledIshak IzharNoch keine Bewertungen
- 4 Flow Chart PretermDokument4 Seiten4 Flow Chart PretermYeni PuspitaNoch keine Bewertungen
- NCP Alzheimers DiseaseDokument2 SeitenNCP Alzheimers DiseaseShawn TejanoNoch keine Bewertungen
- Acute Renal FailureDokument1 SeiteAcute Renal FailureSonia Letran Singson100% (1)
- Jacildo LT Module 6 TCNDokument2 SeitenJacildo LT Module 6 TCNMeryville JacildoNoch keine Bewertungen
- Hyaline Membrane DiseaseDokument31 SeitenHyaline Membrane DiseaseWeng RamojalNoch keine Bewertungen
- Health Assessment: 2 Data Collected During Assessment (Cues)Dokument24 SeitenHealth Assessment: 2 Data Collected During Assessment (Cues)Mabes50% (2)
- General Survey: Mrs. Lalaine Jean D. Lorente, RN, MANDokument15 SeitenGeneral Survey: Mrs. Lalaine Jean D. Lorente, RN, MANHenri Paul LorenteNoch keine Bewertungen
- 2 General ExaminationDokument47 Seiten2 General Examinationzainahalqahtani3Noch keine Bewertungen
- Physical Examination 2011Dokument171 SeitenPhysical Examination 2011Norakmal Andika YusriNoch keine Bewertungen
- Health-Asessment-Finals 2Dokument92 SeitenHealth-Asessment-Finals 2Ebun Rosa100% (1)
- Methods of Clinical ExaminationDokument18 SeitenMethods of Clinical ExaminationPaolo BautistaNoch keine Bewertungen
- Test 3 Study Guide INNATE DEFENSES A&P2Dokument13 SeitenTest 3 Study Guide INNATE DEFENSES A&P2Sarah C. SnooksNoch keine Bewertungen
- AAOS Website ASSIGNMENT CONCEPTS OF FITNESS CLASSDokument2 SeitenAAOS Website ASSIGNMENT CONCEPTS OF FITNESS CLASSSarah C. SnooksNoch keine Bewertungen
- PEBC Test 1 CONCEPTS OF FITNESS W/ ANSWERSDokument13 SeitenPEBC Test 1 CONCEPTS OF FITNESS W/ ANSWERSSarah C. Snooks100% (4)
- Jarvis 12 Skin Hair NailsDokument11 SeitenJarvis 12 Skin Hair NailsSarah C. SnooksNoch keine Bewertungen
- Elektrokardiografi: Prof. Dr. Peter KaboDokument49 SeitenElektrokardiografi: Prof. Dr. Peter KaboRey AlwiwikhNoch keine Bewertungen
- The Heart: Gen PhysioDokument73 SeitenThe Heart: Gen PhysioDawnie AlvarezNoch keine Bewertungen
- Antiarrhythmic DrugsDokument42 SeitenAntiarrhythmic DrugsDr Hotimah HotimahNoch keine Bewertungen
- Cor PulmonaleDokument62 SeitenCor PulmonaleAlbert NixonNoch keine Bewertungen
- Viskin Et Al 2021 Polymorphic Ventricular Tachycardia Terminology Mechanism Diagnosis and Emergency TherapyDokument17 SeitenViskin Et Al 2021 Polymorphic Ventricular Tachycardia Terminology Mechanism Diagnosis and Emergency TherapyMey TalabessyNoch keine Bewertungen
- Basics of ECG: DR Subroto Mandal, MD, DM, DC Associate Professor, CardiologyDokument206 SeitenBasics of ECG: DR Subroto Mandal, MD, DM, DC Associate Professor, CardiologyRavi SharmaNoch keine Bewertungen
- Test Bank Chapter 11: The Pediatric Patient in The Adult Critical Care UnitDokument8 SeitenTest Bank Chapter 11: The Pediatric Patient in The Adult Critical Care UnitAnonymous ZzjzIcmNoch keine Bewertungen
- Current News in Cardiology PDFDokument428 SeitenCurrent News in Cardiology PDFAbel BurleanuNoch keine Bewertungen
- Learning Ecg ModulesDokument150 SeitenLearning Ecg ModulesdodiNoch keine Bewertungen
- Ecg Made EasyDokument343 SeitenEcg Made EasyAbegail IbañezNoch keine Bewertungen
- Family Medicine EORDokument159 SeitenFamily Medicine EORAndrew BowmanNoch keine Bewertungen
- Supplementary Material - ECG TestDokument26 SeitenSupplementary Material - ECG TestSiraj AL sharifNoch keine Bewertungen
- ACLS PharmacologyDokument5 SeitenACLS PharmacologyKim Still ChunnNoch keine Bewertungen
- Acute Myocardial Infarction:: Pathophysiology and PresentationDokument40 SeitenAcute Myocardial Infarction:: Pathophysiology and PresentationSelecta Dejosep GonzalesNoch keine Bewertungen
- Study of The Causes of Mortality in Acute Aluminium Phosphide PoisoningDokument11 SeitenStudy of The Causes of Mortality in Acute Aluminium Phosphide PoisoningHany TawfikNoch keine Bewertungen
- Biphasic DefbrillationDokument16 SeitenBiphasic DefbrillationchanlalNoch keine Bewertungen
- Death CertificateDokument3 SeitenDeath CertificateAllen Peter WeixlerNoch keine Bewertungen
- SVT and DengueDokument4 SeitenSVT and Denguefrengki prasNoch keine Bewertungen
- Common ECG With Management For Family Medicine ResidentsDokument19 SeitenCommon ECG With Management For Family Medicine ResidentsdrhassanashrafeNoch keine Bewertungen
- MCQ PretestDokument3 SeitenMCQ PretestKia AgusputraNoch keine Bewertungen
- The Impact of Coffee Subtypes On Incident Cardiovascular Disease, Arrhythmias, and MortalityDokument10 SeitenThe Impact of Coffee Subtypes On Incident Cardiovascular Disease, Arrhythmias, and MortalityJenny RojoNoch keine Bewertungen