Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (894)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Cook Korean Robin HaDokument176 SeitenCook Korean Robin HaChaitra Reddy100% (1)
- Beyond Meat: A Comparison of The Dietary Intakes of Vegeterian and Non-Vegterian AdolescentsDokument17 SeitenBeyond Meat: A Comparison of The Dietary Intakes of Vegeterian and Non-Vegterian Adolescentsriya chileNoch keine Bewertungen
- Level of Satisfaction of Grade 10 Students on Canteen ServicesDokument20 SeitenLevel of Satisfaction of Grade 10 Students on Canteen ServicesRon Gedor0% (1)
- COMPASS 04-The True Cause of Disease Part 3-Barbara ONeillDokument19 SeitenCOMPASS 04-The True Cause of Disease Part 3-Barbara ONeillJuan P. AlvarezNoch keine Bewertungen
- Detox LGBCleanse PDFDokument2 SeitenDetox LGBCleanse PDFNico LicheNoch keine Bewertungen
- Why 80% of Dieters Fail! - E BookDokument147 SeitenWhy 80% of Dieters Fail! - E BookAvina BharukaNoch keine Bewertungen
- Indicative Development and Management PlanDokument4 SeitenIndicative Development and Management PlanJoseph VillacarlosNoch keine Bewertungen
- Javier, Jomar A. BSN121 Group 83 Nursing Care Plan (Pediatric Patient)Dokument7 SeitenJavier, Jomar A. BSN121 Group 83 Nursing Care Plan (Pediatric Patient)Julie AnnNoch keine Bewertungen
- AHW3e Level 02 Exit TestDokument4 SeitenAHW3e Level 02 Exit TestStephani AmoresNoch keine Bewertungen
- Gut hormones regulating appetiteDokument23 SeitenGut hormones regulating appetiteHeba IyadNoch keine Bewertungen
- Nutrient content of rabbit meat healthier than chicken, beef, porkDokument7 SeitenNutrient content of rabbit meat healthier than chicken, beef, porkjohar MohammadNoch keine Bewertungen
- B Vitamin Deficiencies Symptoms Causes and SolutionsDokument32 SeitenB Vitamin Deficiencies Symptoms Causes and Solutionspantera neagrăNoch keine Bewertungen
- Nutrition Notes: Food Nutrients, Protein Functions and Carbohydrate StructureDokument50 SeitenNutrition Notes: Food Nutrients, Protein Functions and Carbohydrate StructureBelinda ZhangNoch keine Bewertungen
- Planning Sheet For The Third SBA Assignment.Dokument4 SeitenPlanning Sheet For The Third SBA Assignment.FlorenzoNoch keine Bewertungen
- Current ResumeDokument1 SeiteCurrent Resumeapi-650480818Noch keine Bewertungen
- U5Activity8 RosaJavier IA5BDokument3 SeitenU5Activity8 RosaJavier IA5BJafet Mizraim Peraza ChanNoch keine Bewertungen
- Simple PastDokument2 SeitenSimple PastLely IrsanNoch keine Bewertungen
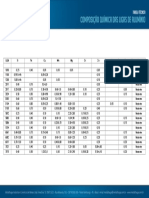
- 1 Composicao Quimica Das Ligas de AluminioDokument1 Seite1 Composicao Quimica Das Ligas de AluminioNorberto A. GhiggiNoch keine Bewertungen
- BSN3D - CABUCOS - ENTREP100 - Activity 9 - Business PlanDokument6 SeitenBSN3D - CABUCOS - ENTREP100 - Activity 9 - Business PlanShane CabucosNoch keine Bewertungen
- Protein Chemistry MCQDokument7 SeitenProtein Chemistry MCQSohaila GodaNoch keine Bewertungen
- Food 5Dokument16 SeitenFood 5Narasimhulu KNoch keine Bewertungen
- 3 ClassDokument7 Seiten3 Classgg alsNoch keine Bewertungen
- Siddeeq Public School: VocabularyDokument6 SeitenSiddeeq Public School: VocabularyHinakhalid50% (2)
- CIP Project Proposal EdittedDokument10 SeitenCIP Project Proposal EdittedFerlizadieflor Fabro De LunasNoch keine Bewertungen
- Ig1 Work Outline For Term 2Dokument5 SeitenIg1 Work Outline For Term 2sisi twumasiNoch keine Bewertungen
- Lesson 2: Matter: One Way of Preventing Non-Biodegradable Materials From Causing Pollution and Harming The EnvironmentDokument2 SeitenLesson 2: Matter: One Way of Preventing Non-Biodegradable Materials From Causing Pollution and Harming The EnvironmentAlexis Dale DiazNoch keine Bewertungen
- Design of A Digital-BasedDokument12 SeitenDesign of A Digital-BasedYoki VirgoNoch keine Bewertungen
- The History and Evolution of Marshmallows from Ancient Egypt to Modern TimesDokument1 SeiteThe History and Evolution of Marshmallows from Ancient Egypt to Modern TimesSushmitha SekarNoch keine Bewertungen
- How To Increase HemoglobinDokument9 SeitenHow To Increase HemoglobinKishore KhudabadiNoch keine Bewertungen
- Tugas Big Chapter 3 Label (Sabtu, 23-92023)Dokument4 SeitenTugas Big Chapter 3 Label (Sabtu, 23-92023)Risma IzamNoch keine Bewertungen