Das könnte Ihnen auch gefallen
- Subarachnoid Block For Caesarean Section in Severe PreeclampsiaDokument6 SeitenSubarachnoid Block For Caesarean Section in Severe PreeclampsiaAndi BintangNoch keine Bewertungen
- Procalcitonin As A Biomarker of Severity Degree in Sepsis Due To PneumoniaDokument5 SeitenProcalcitonin As A Biomarker of Severity Degree in Sepsis Due To PneumoniaAndi BintangNoch keine Bewertungen
- Medical Hypotheses: Yixian Li, Juan Zhou, Ian Burkovskiy, Pollen Yeung, Christian Lehmann TDokument3 SeitenMedical Hypotheses: Yixian Li, Juan Zhou, Ian Burkovskiy, Pollen Yeung, Christian Lehmann TAndi BintangNoch keine Bewertungen
- Parthasarathy2013 PDFDokument7 SeitenParthasarathy2013 PDFAndi BintangNoch keine Bewertungen
- Bar A Zanchi 2018Dokument17 SeitenBar A Zanchi 2018Andi BintangNoch keine Bewertungen
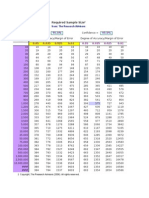
- Required Sample Size: From: The Research AdvisorsDokument3 SeitenRequired Sample Size: From: The Research AdvisorsAbhishek Sharma100% (1)
- Cultural Sociology of Mental Illness n28Dokument5 SeitenCultural Sociology of Mental Illness n28Andi BintangNoch keine Bewertungen
- Overweight linked to increased risk of lower back painDokument8 SeitenOverweight linked to increased risk of lower back painAndi BintangNoch keine Bewertungen
- Anestesia General para Césarea PDFDokument7 SeitenAnestesia General para Césarea PDFAgnese ValentiniNoch keine Bewertungen
- 1 s2.0 S1052305714000561 MainDokument6 Seiten1 s2.0 S1052305714000561 MainAndi BintangNoch keine Bewertungen
- Anestesia General para Césarea PDFDokument7 SeitenAnestesia General para Césarea PDFAgnese ValentiniNoch keine Bewertungen
- Depresión e InmunidadDokument13 SeitenDepresión e InmunidadgabisaenaNoch keine Bewertungen
- Hepatitis C APASLfghDokument27 SeitenHepatitis C APASLfghAndi BintangNoch keine Bewertungen
- Sacral Nerve Stimulation Reduces Elevated Urinary Nerve Growth Factor Levels in Women With Symptomatic Detrusor OveractivityDokument5 SeitenSacral Nerve Stimulation Reduces Elevated Urinary Nerve Growth Factor Levels in Women With Symptomatic Detrusor OveractivityAndi BintangNoch keine Bewertungen
- 1 s2.0 S0002937803001388 MainDokument3 Seiten1 s2.0 S0002937803001388 MainAndi BintangNoch keine Bewertungen
- Association Between Constipation and Colorectal Cancer Systematic Review and Meta-Analysis of Observational StusdgdiesDokument10 SeitenAssociation Between Constipation and Colorectal Cancer Systematic Review and Meta-Analysis of Observational StusdgdiesAndi BintangNoch keine Bewertungen
- Instruction For Author ClimactericDokument9 SeitenInstruction For Author ClimactericAndi BintangNoch keine Bewertungen
- 2013 Student Membership ApplicationDokument1 Seite2013 Student Membership ApplicationAndi BintangNoch keine Bewertungen
- 1 s2.0 S0002937803001388 MainDokument3 Seiten1 s2.0 S0002937803001388 MainAndi BintangNoch keine Bewertungen
- 1 s2.0 S0002937800704534 Main PDFDokument1 Seite1 s2.0 S0002937800704534 Main PDFAndi BintangNoch keine Bewertungen
- Prevalence of Diabetes and Impaired Fasting Glucose in Adults in The U.S. PopulationDokument6 SeitenPrevalence of Diabetes and Impaired Fasting Glucose in Adults in The U.S. PopulationAndi BintangNoch keine Bewertungen
- 1 s2.0 S0021755713002003 MainDokument6 Seiten1 s2.0 S0021755713002003 MainAndi BintangNoch keine Bewertungen
- Serviks DocjhjuDokument366 SeitenServiks DocjhjuAndi BintangNoch keine Bewertungen
- Anthropometry: Ergonomics Additional ResourcesDokument5 SeitenAnthropometry: Ergonomics Additional ResourcesAndi BintangNoch keine Bewertungen
- 1 s2.0 S0021755713002003 MainDokument6 Seiten1 s2.0 S0021755713002003 MainAndi BintangNoch keine Bewertungen
- MK Giz Slide Infant Feeding PracticeDokument1 SeiteMK Giz Slide Infant Feeding PracticeAndi BintangNoch keine Bewertungen
- PCT CAP ABiuytoDokument10 SeitenPCT CAP ABiuytoAndi BintangNoch keine Bewertungen
- Urologi PDFDokument237 SeitenUrologi PDFAndi BintangNoch keine Bewertungen
- ATS Guidelines CAP ManagementDokument25 SeitenATS Guidelines CAP ManagementMae Matira AbeladorNoch keine Bewertungen
- Cap Bts 2009 ComplitdgDokument139 SeitenCap Bts 2009 ComplitdgAndi BintangNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5782)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (72)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Morphological Variation of The Maxillary Lateral Incisor: SciencedirectDokument8 SeitenMorphological Variation of The Maxillary Lateral Incisor: SciencedirectKanish AggarwalNoch keine Bewertungen
- Spa Multiple PrincipalDokument2 SeitenSpa Multiple PrincipalGn67% (3)
- Dog Training Book Rex in The CityDokument56 SeitenDog Training Book Rex in The CitybebekbuluhNoch keine Bewertungen
- Basic Knowledge About Radio Network: Viettel Networks Corporation - O0oDokument34 SeitenBasic Knowledge About Radio Network: Viettel Networks Corporation - O0ovilaphong vongphachithNoch keine Bewertungen
- ACHE Fin Fan TechDokument15 SeitenACHE Fin Fan TechAnonymous 8Mc8boONNoch keine Bewertungen
- OUR Company: MGT 351 Presentation On Human Resource PlanDokument16 SeitenOUR Company: MGT 351 Presentation On Human Resource Planaparajita promaNoch keine Bewertungen
- Lesson 2 Professionals and Practitioners in CounselingDokument93 SeitenLesson 2 Professionals and Practitioners in CounselingDaneNoch keine Bewertungen
- People Vs Gona, G.R. No. 32066Dokument2 SeitenPeople Vs Gona, G.R. No. 32066Johnric PandacNoch keine Bewertungen
- 02 - Motor PDFDokument80 Seiten02 - Motor PDFRenato Assis da SilvaNoch keine Bewertungen
- 2200A Series1Dokument1 Seite2200A Series1cvrao90Noch keine Bewertungen
- ProcrastinationDokument8 SeitenProcrastinationPracheeNoch keine Bewertungen
- Activities For FinalsDokument10 SeitenActivities For FinalsAmbita CherylNoch keine Bewertungen
- CAFAM BasicReportDokument135 SeitenCAFAM BasicReportDaniel R. CC AIRESNoch keine Bewertungen
- Sample COVID19 Plan For Small EmployersDokument6 SeitenSample COVID19 Plan For Small EmployersLou Darryl S. GamboaNoch keine Bewertungen
- Castle On The HillDokument2 SeitenCastle On The HillRica Marie PadronesNoch keine Bewertungen
- Proposal Tripurainfo Job PortalDokument10 SeitenProposal Tripurainfo Job PortalEkta DevNoch keine Bewertungen
- Final Study SS of 2nd PB 2023Dokument65 SeitenFinal Study SS of 2nd PB 2023rahul SNoch keine Bewertungen
- Cell Counting Neubauer ChamberDokument6 SeitenCell Counting Neubauer ChamberHerma ZulaikhaNoch keine Bewertungen
- MULTIPLE CHOICE-ComputationalDokument5 SeitenMULTIPLE CHOICE-Computationaljie calderonNoch keine Bewertungen
- Effect of Authoritarian2Dokument10 SeitenEffect of Authoritarian2Zarghoona inayatNoch keine Bewertungen
- Bexley Selection Tests Specimen Questions - Verbal ReasoningDokument8 SeitenBexley Selection Tests Specimen Questions - Verbal Reasoningpflora41Noch keine Bewertungen
- BIOLOGYDokument11 SeitenBIOLOGYElla May TimoteoNoch keine Bewertungen
- Filipino Personality and Culture TraitsDokument2 SeitenFilipino Personality and Culture TraitsAva Marie Lampad - CantaNoch keine Bewertungen
- Mohr SALT CHEAT SHEETDokument3 SeitenMohr SALT CHEAT SHEETpriyanshu jain100% (1)
- NFDN 2005 Report On Progress of Professional PortlioDokument4 SeitenNFDN 2005 Report On Progress of Professional Portlioapi-328324207Noch keine Bewertungen
- G8 en La Evaluación GeriátricaDokument12 SeitenG8 en La Evaluación GeriátricaMIGUEL MORENONoch keine Bewertungen
- Chemical and Enzymatic Synthesis of LanthioninesDokument15 SeitenChemical and Enzymatic Synthesis of LanthioninesSam SonNoch keine Bewertungen
- BS EN 206-1 and BS 8500 Concrete Standards GuideDokument23 SeitenBS EN 206-1 and BS 8500 Concrete Standards GuideJasmine SmithNoch keine Bewertungen
- LotusEliseS1 ServiceManualDokument626 SeitenLotusEliseS1 ServiceManualClive BuckberryNoch keine Bewertungen
- Stage Fright: Its Experience As A Problem and Coping With ItDokument11 SeitenStage Fright: Its Experience As A Problem and Coping With ItcabatinganacieNoch keine Bewertungen