Das könnte Ihnen auch gefallen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Malalignment Syndrome - Implications For Medicine and Sport PDFDokument455 SeitenThe Malalignment Syndrome - Implications For Medicine and Sport PDFIvaylo Marinov100% (1)
- Anatomy MnemonicsDokument7 SeitenAnatomy MnemonicsUlfatul UlyaNoch keine Bewertungen
- Anterior Cruciate Ligament InjuryDokument30 SeitenAnterior Cruciate Ligament InjuryyohanNoch keine Bewertungen
- WCT Workout TemplateDokument5 SeitenWCT Workout TemplateRami0% (2)
- Earle Liederman Course 8-13-2008 - 2Dokument133 SeitenEarle Liederman Course 8-13-2008 - 2Rappadappa100% (2)
- Basic Taekwondo Techniques and TerminologyDokument111 SeitenBasic Taekwondo Techniques and TerminologyGabriel FariaNoch keine Bewertungen
- List of Anatomy Mnemonics - WikipediaDokument33 SeitenList of Anatomy Mnemonics - WikipediaSudeepthiNoch keine Bewertungen
- Principais Sistemas Do OrganismoDokument5 SeitenPrincipais Sistemas Do OrganismoDiana VieiraNoch keine Bewertungen
- Anp 1106 Midterm 1 NotesDokument10 SeitenAnp 1106 Midterm 1 NotesKristyNoch keine Bewertungen
- Reactive Wall Push-Up: ExecutionDokument36 SeitenReactive Wall Push-Up: Executioncoach_noeNoch keine Bewertungen
- HEALTH ASSESSMENT - Breasts & Regional LymphaticsDokument5 SeitenHEALTH ASSESSMENT - Breasts & Regional LymphaticsMich Hiel OforraNoch keine Bewertungen
- Mechanism of LaborDokument5 SeitenMechanism of LaborHeron EgretNoch keine Bewertungen
- Acl Reconstruction Rehab ProtocolDokument35 SeitenAcl Reconstruction Rehab ProtocolCesar OliverosNoch keine Bewertungen
- Resistance Band Exercises CompleteDokument9 SeitenResistance Band Exercises CompleteDani ListerNoch keine Bewertungen
- The Painful Shoulder - Part I. Clinical Evaluation. - American Family PhysicianDokument16 SeitenThe Painful Shoulder - Part I. Clinical Evaluation. - American Family PhysicianAdalberto GomesNoch keine Bewertungen
- Pathological Conditions of Musculoskeletal SystemDokument28 SeitenPathological Conditions of Musculoskeletal SystemNipun ShamikaNoch keine Bewertungen
- Best Breastfeeding Positions by StageDokument3 SeitenBest Breastfeeding Positions by StageAngelie Estilo Sarabia PacienteNoch keine Bewertungen
- Anatomy Review of Extreme TiesDokument65 SeitenAnatomy Review of Extreme Tiesskihard0404749Noch keine Bewertungen
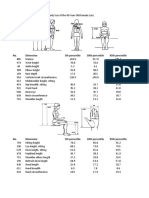
- Human Factors Data PDFDokument9 SeitenHuman Factors Data PDFBalram JhaNoch keine Bewertungen
- Is Video-Based Education An Effective Method in Surgical Education? A Systematic ReviewDokument9 SeitenIs Video-Based Education An Effective Method in Surgical Education? A Systematic Reviewmuhikhsan marikharNoch keine Bewertungen
- GOOD ONE - Posterior Tibialis ExercisesDokument2 SeitenGOOD ONE - Posterior Tibialis ExercisesSylvia GraceNoch keine Bewertungen
- Management Update: Knee & Shoulder InjuriesDokument43 SeitenManagement Update: Knee & Shoulder InjuriesChairiniFikryNoch keine Bewertungen
- A Person Is Performing Slow Arm Curls With A 10-Kg Weight As - QuizletDokument5 SeitenA Person Is Performing Slow Arm Curls With A 10-Kg Weight As - Quizlet刘洋Noch keine Bewertungen
- Standing Dumbbell One-Leg Calf Raise: Exercise DetailsDokument3 SeitenStanding Dumbbell One-Leg Calf Raise: Exercise DetailsDavid RomeroNoch keine Bewertungen
- Anatomy Forum LLDoneDokument5 SeitenAnatomy Forum LLDoneMedShareNoch keine Bewertungen
- Foot and Ankle Surgery: Francesco Di Caprio, MD, Renato Meringolo, MD, Marwan Shehab Eddine, MD, Lorenzo Ponziani, MDDokument7 SeitenFoot and Ankle Surgery: Francesco Di Caprio, MD, Renato Meringolo, MD, Marwan Shehab Eddine, MD, Lorenzo Ponziani, MDNishanthini AnnamalaiNoch keine Bewertungen
- World Breastfeeding Week UntouchedDokument4 SeitenWorld Breastfeeding Week UntouchedSowbharnikaNoch keine Bewertungen
- EBP Literature Searching SkillsDokument47 SeitenEBP Literature Searching SkillsAndi sutandiNoch keine Bewertungen
- 10y Reflection of Sport Clinic - Dr. Damayanti Tinduh, DR., SP - KFR (K)Dokument34 Seiten10y Reflection of Sport Clinic - Dr. Damayanti Tinduh, DR., SP - KFR (K)dewifebrianaNoch keine Bewertungen
- Lamaze Session 3Dokument32 SeitenLamaze Session 3Andrea Olimpia PopNoch keine Bewertungen