Das könnte Ihnen auch gefallen
- Slide Kuliah Transfusi DarahDokument31 SeitenSlide Kuliah Transfusi Darahfenti nurul khafifahNoch keine Bewertungen
- Principles of Transfusion in Liver DiseasesDokument38 SeitenPrinciples of Transfusion in Liver DiseasesNallagondla ThulasiramNoch keine Bewertungen
- Hemostatic Strategies For Minimizing Mortality in Major Blood LossDokument26 SeitenHemostatic Strategies For Minimizing Mortality in Major Blood LossJonathan wiradinataNoch keine Bewertungen
- Clinical Indications For Platelets: Key MessagesDokument4 SeitenClinical Indications For Platelets: Key MessagesKristian WilsonNoch keine Bewertungen
- 7 3 Transfusion Management of Major HaemorrhageDokument6 Seiten7 3 Transfusion Management of Major HaemorrhageKoas Neuro UnpattiNoch keine Bewertungen
- Transfusion Guidelines HemDokument4 SeitenTransfusion Guidelines HemnandhinisankaranNoch keine Bewertungen
- BLOOD - FinalDokument8 SeitenBLOOD - FinalanuNoch keine Bewertungen
- 7: Effective Transfusion in Surgery and Critical CareDokument16 Seiten7: Effective Transfusion in Surgery and Critical CareNick-Hugh Sean WisdomNoch keine Bewertungen
- Blood Transfusion.Dokument23 SeitenBlood Transfusion.Madalina TalpauNoch keine Bewertungen
- Practice Guidelines For Perioperative Blood Management An Updated Report by The American Society of Anesthesiologists Task Force OnDokument13 SeitenPractice Guidelines For Perioperative Blood Management An Updated Report by The American Society of Anesthesiologists Task Force OnMadalina TalpauNoch keine Bewertungen
- CMQCC - Transfusion in Obstetric HemorrhageDokument10 SeitenCMQCC - Transfusion in Obstetric HemorrhageBerri RahmadhoniNoch keine Bewertungen
- Bleeding & Coagulopathies in Clinical CareDokument20 SeitenBleeding & Coagulopathies in Clinical CareKarina Mega WNoch keine Bewertungen
- Blood Transfusion in Hemorrhagic ShockDokument28 SeitenBlood Transfusion in Hemorrhagic Shocklas100% (2)
- Blood Transfusion SeminarDokument58 SeitenBlood Transfusion SeminarsharewdelelegnNoch keine Bewertungen
- Massive Transfusion Protocol 2017Dokument9 SeitenMassive Transfusion Protocol 2017RosNoch keine Bewertungen
- 9 Transfusion Guidelines 2006Dokument6 Seiten9 Transfusion Guidelines 2006Melania OanaNoch keine Bewertungen
- Appropriate Use of Blood Components: Clinical Practice GuidelinesDokument2 SeitenAppropriate Use of Blood Components: Clinical Practice GuidelinesEstefani BlancoNoch keine Bewertungen
- Upper GI BleedDokument8 SeitenUpper GI BleedbbyesNoch keine Bewertungen
- Blood Transfusion 2Dokument12 SeitenBlood Transfusion 2Helene AlawamiNoch keine Bewertungen
- Jurnal AkiDokument7 SeitenJurnal AkiNining Komala SariNoch keine Bewertungen
- Blood Component TherapyDokument73 SeitenBlood Component TherapySaikat Prasad DattaNoch keine Bewertungen
- Blood Transfusion 3.0Dokument1 SeiteBlood Transfusion 3.0kimglaidyl bontuyanNoch keine Bewertungen
- TIVA in CKDDokument7 SeitenTIVA in CKDfixheartNoch keine Bewertungen
- Managing Coagulopathy ICUDokument38 SeitenManaging Coagulopathy ICUMirabela Colac100% (1)
- Blood Transfusion in OBSDokument7 SeitenBlood Transfusion in OBSDr-Saja O. DmourNoch keine Bewertungen
- Blood Components Dosage and Their Administration (Compatibility Mode)Dokument7 SeitenBlood Components Dosage and Their Administration (Compatibility Mode)Chandra SekarNoch keine Bewertungen
- Use of Blood Products in The Critically IllDokument25 SeitenUse of Blood Products in The Critically IllAna María Díaz MedinaNoch keine Bewertungen
- Bleeding in A NeonateDokument36 SeitenBleeding in A NeonateDrBibek AgarwalNoch keine Bewertungen
- PBM (Autosaved)Dokument36 SeitenPBM (Autosaved)dr AmitNoch keine Bewertungen
- Adult Blood Transfusion MedicsDokument15 SeitenAdult Blood Transfusion MedicsStanislaus JosephNoch keine Bewertungen
- Blood Transfusion - Indications, Administration and Adverse Reactions PDFDokument9 SeitenBlood Transfusion - Indications, Administration and Adverse Reactions PDFStacey WoodsNoch keine Bewertungen
- Blood Component Therapy-4th Year MSDokument22 SeitenBlood Component Therapy-4th Year MSAyu Roossea MustikaNoch keine Bewertungen
- Use of Blood Products in The Critically Ill - UpToDateDokument13 SeitenUse of Blood Products in The Critically Ill - UpToDateOscar F RojasNoch keine Bewertungen
- Addison K May, MD John P Reilly, MD, Msce Scott Manaker, MD, PHD Arthur J Silvergleid, MD Geraldine Finlay, MD Contributor DisclosuresDokument12 SeitenAddison K May, MD John P Reilly, MD, Msce Scott Manaker, MD, PHD Arthur J Silvergleid, MD Geraldine Finlay, MD Contributor DisclosuresAlvaro HaroNoch keine Bewertungen
- Anaesthesia Practice Newsletter Isue 58Dokument8 SeitenAnaesthesia Practice Newsletter Isue 58muhammad shahrozeNoch keine Bewertungen
- 2013 BloodUsageCardDokument4 Seiten2013 BloodUsageCardtonnywongsoNoch keine Bewertungen
- CRRT Guidelines RenalDokument5 SeitenCRRT Guidelines Renalanon_361066654100% (1)
- Blood ConservationDokument21 SeitenBlood ConservationfraolNoch keine Bewertungen
- Blood TransfusionDokument104 SeitenBlood TransfusionrodelagapitoNoch keine Bewertungen
- Blood ProductsDokument70 SeitenBlood Productsjadhamade339Noch keine Bewertungen
- Artikel Tramed InfusDokument7 SeitenArtikel Tramed InfusZsa Zsa OllyviaNoch keine Bewertungen
- Bleeding and TransfusionDokument32 SeitenBleeding and TransfusionWalid KuncoroNoch keine Bewertungen
- Blood Transfusion Notes For StudentsDokument5 SeitenBlood Transfusion Notes For StudentsMegan TurnerNoch keine Bewertungen
- Blood Components: D.) Washed Rbcs and Frozen/Deglycerolized RbcsDokument3 SeitenBlood Components: D.) Washed Rbcs and Frozen/Deglycerolized RbcsGerarld Immanuel KairupanNoch keine Bewertungen
- Bloody Easy PDFDokument164 SeitenBloody Easy PDFJenny JeongNoch keine Bewertungen
- Seminar Y3B2 - Transfusion of Blood & Blood Products - 20240306 - 112523 - 0000Dokument53 SeitenSeminar Y3B2 - Transfusion of Blood & Blood Products - 20240306 - 112523 - 0000malekNoch keine Bewertungen
- 11 Peri Operative CareDokument43 Seiten11 Peri Operative CareAdnan MaqboolNoch keine Bewertungen
- Pediatric Hematology Oncology Ward Officer HandbookDokument40 SeitenPediatric Hematology Oncology Ward Officer HandbookLetchumana KrishnanNoch keine Bewertungen
- Postpartum HaemorrhageDokument44 SeitenPostpartum Haemorrhageella_28Noch keine Bewertungen
- Citrate in CRRTDokument8 SeitenCitrate in CRRTAshish PandeyNoch keine Bewertungen
- Blood ProductsDokument2 SeitenBlood ProductstechnoelfyNoch keine Bewertungen
- Blood and Blood Product (F)Dokument50 SeitenBlood and Blood Product (F)bharat singhNoch keine Bewertungen
- Therapeutic Apheresis Guideline FINALVERSION7 THAPRIL15Dokument47 SeitenTherapeutic Apheresis Guideline FINALVERSION7 THAPRIL15RalucaNoch keine Bewertungen
- Disseminated Intravascular CoagulationDokument10 SeitenDisseminated Intravascular Coagulationkep1313Noch keine Bewertungen
- Bloodproducttransfusions Andreactions: Jessica L. Osterman,, Sanjay AroraDokument12 SeitenBloodproducttransfusions Andreactions: Jessica L. Osterman,, Sanjay AroraAdi ParamarthaNoch keine Bewertungen
- Transfusion in Specfic SituationsDokument42 SeitenTransfusion in Specfic SituationsAhmed EshraNoch keine Bewertungen
- Blood ProductsDokument41 SeitenBlood ProductsrijjorajooNoch keine Bewertungen
- Postoperative Hemorrhagic Shock Class Iii Following Transurethral Resection of The Prostate (Turp) PatientDokument20 SeitenPostoperative Hemorrhagic Shock Class Iii Following Transurethral Resection of The Prostate (Turp) Patientanang raharjoNoch keine Bewertungen
- Vox SanguinisDokument179 SeitenVox SanguinistristanmunarNoch keine Bewertungen
- Alternatives to Blood Transfusion in Transfusion MedicineVon EverandAlternatives to Blood Transfusion in Transfusion MedicineAlice ManiatisNoch keine Bewertungen
- Instrumentation & Measurement SystemsDokument7 SeitenInstrumentation & Measurement SystemsAnkit KumarNoch keine Bewertungen
- Brochure E-AIR T400-900 WEG APP 2958 1020 02 ENDokument3 SeitenBrochure E-AIR T400-900 WEG APP 2958 1020 02 ENDaniel BravoNoch keine Bewertungen
- Compound Wall Toilet Revised (4) - ModelDokument1 SeiteCompound Wall Toilet Revised (4) - ModelInfra SupportNoch keine Bewertungen
- Examination Speaking Assignments Term III - 2021Dokument2 SeitenExamination Speaking Assignments Term III - 2021Khrystyna ShkilniukNoch keine Bewertungen
- Hypochondriasis and Health Anxiety - A Guide For Clinicians (PDFDrive)Dokument289 SeitenHypochondriasis and Health Anxiety - A Guide For Clinicians (PDFDrive)Fernanda SilvaNoch keine Bewertungen
- PEPSIDokument99 SeitenPEPSIkingloiyaNoch keine Bewertungen
- MCQ Rewriting 1Dokument10 SeitenMCQ Rewriting 1Quỳnh Anh NguyễnNoch keine Bewertungen
- Dell Inspiron 16 5000 (5625) Laptop - Dell IndiaDokument5 SeitenDell Inspiron 16 5000 (5625) Laptop - Dell IndiamubbunNoch keine Bewertungen
- Yamaha MG16 PDFDokument2 SeitenYamaha MG16 PDFmiskoyu027Noch keine Bewertungen
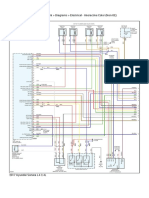
- 2017 Hyundai Sonata L4-2.4L Engine Controls (Powertrain Management) - ALLDATA RepairDokument6 Seiten2017 Hyundai Sonata L4-2.4L Engine Controls (Powertrain Management) - ALLDATA RepairChino PlagaNoch keine Bewertungen
- Cleavage in MammalsDokument51 SeitenCleavage in MammalsIrfan Azram100% (4)
- Effect of Calorie Restriction and Exercise On Type 2 DiabetesDokument18 SeitenEffect of Calorie Restriction and Exercise On Type 2 DiabetesDitya Monica 065Noch keine Bewertungen
- YS 700W Bifacial Solar PanelDokument2 SeitenYS 700W Bifacial Solar PanelDaniel RodriguezNoch keine Bewertungen
- Bendable ConcreteDokument21 SeitenBendable ConcreteJulia Sebastian0% (1)
- Benzene and Phenol (25-05-2023)Dokument55 SeitenBenzene and Phenol (25-05-2023)hibajama72Noch keine Bewertungen
- ASTM E 1066 - 95 Standard Practice For Ammonia Colorimetric Leak Testing PDFDokument5 SeitenASTM E 1066 - 95 Standard Practice For Ammonia Colorimetric Leak Testing PDFАртем ТитовNoch keine Bewertungen
- Urgent Medical Device CorrectionDokument4 SeitenUrgent Medical Device CorrectionVladimir OsunaNoch keine Bewertungen
- Ornament of Clear RealizationDokument11 SeitenOrnament of Clear RealizationPrachi AryaNoch keine Bewertungen
- Valvula Reguladoras Pilotados DANFOSSDokument2 SeitenValvula Reguladoras Pilotados DANFOSSJurandir Laureano SILVA JUNIORNoch keine Bewertungen
- Theory-Set & Relations PDFDokument4 SeitenTheory-Set & Relations PDFmp SinghNoch keine Bewertungen
- Catálogo DP InglêsDokument20 SeitenCatálogo DP Inglêsjf2003Noch keine Bewertungen
- Pakistan PresentationDokument17 SeitenPakistan PresentationYaseen Khan100% (1)
- Proyector SNF 111Dokument3 SeitenProyector SNF 111Liliana Patricia PederneraNoch keine Bewertungen
- Unusual and Marvelous MapsDokument33 SeitenUnusual and Marvelous MapsRajarajan100% (1)
- Brochure - Citadines Flatiron Phnom Penh - EnglishDokument4 SeitenBrochure - Citadines Flatiron Phnom Penh - EnglishTix VirakNoch keine Bewertungen
- Wolfi Landstreicher - Willful Disobedience - Number 3Dokument32 SeitenWolfi Landstreicher - Willful Disobedience - Number 3populaererNoch keine Bewertungen
- Standard MissileDokument2 SeitenStandard Missilemadox_3m100% (1)
- Portable Load Banks: CressallDokument1 SeitePortable Load Banks: CressallYashveer26Noch keine Bewertungen
- Trucks Fin Eu PCDokument117 SeitenTrucks Fin Eu PCjeanpienaarNoch keine Bewertungen
- PerthDokument21 SeitenPerthjohn_wlmns3929Noch keine Bewertungen