Abstract The purpose of the research was to explore a combined semantic + multimodal communication program (S+MCP) for an individual
with chronic moderate-severe aphasia with coexisting semantic deficits. The effect of S+MCP on his ability to switch between modalities when an initial communication attempt failed was examined during a referential communication task and administration of the CADL-2 with modified scoring. The participant demonstrated increased switching behavior between modalities during both tasks, and increased use of combined modalities (e.g., verbal plus gesture). Clinical implications and future research are discussed.
Effects of Semantic + Multimodal Communication Program for Switching Behavior in Moderate-Severe Aphasia Word retrieval deficits are a hallmark characteristic of aphasia. According to a model of lexical retrieval hypothesized by Dell and colleagues (2004), retrieval of an object name involves a two-step process: 1) lemma access, the connection of a concept to a semantic representation of a word, and 2) phonological access, connecting the lemma to the phonological form of the word resulting in verbal expression. Many clinicians provide instruction in alternative modalities to compensate for deficits in the second step. Multimodal interventions incorporating many alternative modalities may be introduced to improve overall communicative effectiveness (e.g., Rodriguez, Raymer & Rothi, 2006). Despite the ability of people with aphasia to learn to produce their alternative modalities, some people may not attempt to switch to an alternate communication modality when verbal output fails (Purdy, Duffy, & Coelho, 1994). A Multimodal Communication Program (MCP) was developed to teach communication modalities simultaneously to improve the ability of people with aphasia to switch to an alternate modality when a communication attempt fails (Purdy & VanDyke, 2011). Preliminary investigations of MCP revealed that coexisting semantic deficits may affect the outcome. The purpose of the current study was to investigate the efficacy of a combined semantic and multimodal communication program (S+MCP) for people with moderate-severe aphasia that exhibit semantic deficits. S+MCP aims to address deficits the both steps of lexical access to improve the overall communicative effectiveness through increased alternative modality production and switching behavior. Method Participant The participant was a 77-year-old male with chronic severe global aphasia resulting from a single left-hemisphere stroke. The participant was a native speaker of American English, righthanded prior to the stroke, and passed vision and hearing screenings. He also had a documented semantic impairment as determined by a raw score below 40 out of a 52 on the Pyramids and Palm Trees Test (PPT) (Howard & Patterson, 1992). Table 1 contains the participants demographic information and initial assessment data. Materials Thirty target nouns commonly used in American English were randomly divided into three lists of ten words each and were represented by three image sets. One set of 30 colored line drawings was used by the communication partner during the Referential Communication Task (RCT) probes and during the S+MCP treatment sessions. A second set of 30 colored line drawings was used to create three communication boards consisting of two horizontal rows of five items each printed on standard letter paper. The examiner showed a third set of 30 color photographs representing all target words to the participant during the RCT. White 4X6 inch index cards containing written text of treated words, semantic features, and semantic feature foils in 32 point Arial font were used during semantic treatment. The participant had access to paper and a marker during all sessions.
Experimental Design and Procedure The researchers implemented a multiple baseline design across stimuli (word lists) to examine the affects of S+MCP on participants switching behavior. The dependent variable was the RCT communicative flexibility score defined as the percentage of successful modality switches out of the total number of opportunities to switch modalities. A secondary dependent variable was the CADL-2 communicative flexibility score (Purdy & Koch, 2006) measured pre and post intervention. Experimental sessions included baseline, intervention and postintervention sessions. First, formal assessments were administered across five baseline sessions. The participant completed the RCT probe with all 30 words during each baseline session and prior to the first treatment session for a total of six pretreatment probes. The RCT probe involved the examiner, the participant, and a trained communication partner. The examiner presented a photograph depicting a target word to the participant. The participant was instructed to communicate the word to the communication partner who was unable to see the photograph. Pen and paper for writing and drawing, as well as a communication board were available to the participant. Following the initial production by the participant, the communication partner presented either a correct or incorrect colored line drawing based on the response of the participant and whether it was an item predetermined to promote switching behavior. To promote switching behavior by the participant, the communication partner purposefully provided an incorrect item 50% of the time (5 target words from each list) regardless of the participants response. The purpose of the RCT was to determine if the participant was able to switch modalities to repair a communication breakdown that occurred during the first communication attempt. Each intervention session began with the RCT probe. Treatment sessions included two phases; during each phase the examiner provided treatment for ten words on one treatment word list (Treatment list 1 or Treatment list 2). The participant completed a semantic treatment followed by MCP for each treated word prior to proceeding to the subsequent word. For the semantic treatment, the examiner presented the participant with a colored line drawing of the target word paired with orthographic representation of the target word. The participant was presented with three features: one related to the target word and two unrelated foils. The examiner read each feature answer choice and requested that the participant place the correct semantic feature with the target word. The participant sorted the target word three times, once for each of three types of semantic features: category, location, and property. MCP began with presentation of a colored line drawing depicting one of the 10 treated words. The examiner modeled each of three modalities to depict the pictured concept. After the participant imitated each behavior, he was instructed to produce the three modalities for the target word, given verbal or gestural cueing as needed. Then, the participant produced all three modalities a second time in a communicative scenario with the examiner. Based on performance during the RCT and the participant and caregivers stated preference, the researchers selected
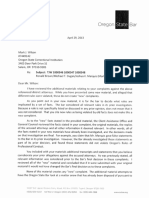
speaking, pointing to the communication board, gesturing, and drawing as intervention modalities. After completion of the two phases of intervention, the participant completed three sessions of post-treatment assessments and the RCT probe. The participant completed the RCT and an assessment of his ability to produce each modality for each target word during each of the three post-intervention sessions. Results Following S+MCP, the participant demonstrated increased switching behavior during the RCT probe and CADL-2. Communicative flexibility scores during RCT probes and CADL-2 are available in Figures 1 and 2, respectively. Unexpectedly, the researchers also observed changes in the frequency with which the participant combined communication modalities following MCP (speaking and gesturing simultaneously). Figure 3 shows the changes in the participants use of combined modalities. Finally, Table 2 contains the participants pre/post assessment data. Discussion The results suggest that for some people with aphasia who have significant semantic impairments, a combined S+MCP intervention may increase switching among alternative modalities to repair communication breakdowns. However, as evidenced by the delayed increase in switching behavior, the researchers concluded that some people might need additional intervention sessions to master switching behavior in a communicative task. Finally, further investigation of various aspects of communicative flexibility is warranted given the unexpected increase in combined modality use.
References Dell, G.S., Lawler, E.N., Harris, H.D., & Gordon, J.K. (2004). Models of errors of omission in aphasic naming. Cognitive Neurophychology, 21, 125-145. Helm-Estabrooks, N. (2001). Cognitive Linguistic Quick Test. San Antonio, TX: The Psychological Corporation. Holland, A., Frattali, C., & Fromm, D. (1999). Communication Activities of Daily Living, Second Edition. Howard, D., & Patterson, K. (1992). The Pyramids and Palm Trees Test. Bury St. Edmunds, UK: Thames Valley Test Company. Kay, J., Lesser, R. and Coltheart, M., 1992, The Psycholinguistic Assessment of Language Processing in Aphasia. Hove: Lawrence Erlbaum Associates. Kertesz, A. (2006). Western Aphasia Battery. New York: The Psychological Corporation. Purdy, M., Duffy, R.J., & Coelho, C.A. (1994). An investigation of the communicative use of trained symbols following multimodality training. Clinical Aphasiology, 22, 345-356. Purdy, M, & Van Dyke, J.A. (2011). Multimodal communication training in aphasia: A pilot study. Journal of Medical Speech-Language Pathology, 19, 45-58. Rodriguez, A., Raymer, A., & Rothi, L. (2006). Effects of gesture + verbal and semanticphonologic treatments for verb retrieval in aphasia. Aphasiology, 20, 286-297.
Table 1 Participant Characteristics Western Aphasia BatteryRevised (Aphasia Quotient) Pyramids and Palm Trees Test Time Post Stroke Motor Status Education Cognitive Linguistic Quick Test Clock Drawing Subtest Symbol Trails Subtest Reading Comprehension Battery for Aphasia Subtest I: WordVisual Subtest II: WordAuditory 19.7 28/52 15 months Right hemiparesis; Ambulatory 16 years 1/13 0/10 6/10 6/10
Table 2 Pre- and Post-Treatment Test Scores Communicative Activities of Daily Living-2 Pyramids and Palm Trees Test Weschler Memory Scale-III: Spatial Span Subtest* Forward Backward Psycholinguistic Assessment of Language Processing in Aphasia Subtest 47: Spoken Word Picture Matching Subtest 48: Written Word Picture Matching Subtest 51: Word Semantic AssociationHigh Imageability Words Ravens Coloured Progressive Matrices Baseline 35/100 28/52 4/16 4/16 19/40 16/40 4/15 Post-Treatment 30/100 44/52 4/16 3/16 22/40 14/40 4/15
29/37
27/37
*Used as a control measure as the researchers did not expect S+MCP to affect the participants memory.
Figure 1 Participants Communicative Flexibility Scores on RCT Baseline 80 Communicative Flexibility Score (Percentage) 70 60 50 40 30 20 10 Treated List 1 Treated List 2 Untreated List Treatment Phase 1 Treatment Phase 2 Post-Treatment
0
1 2 3 4 5 6 7 8 9 10 11 12 Sessions 13 14 15 16 17 18 19 20
*Commutative flexibility score = number of modality switches out of the number of opportunities to switch .
Figure 2 Participants Communicative Flexibility Scores on CADL-2 Baseline
45
Post-Treatment
Communicative Flexibiltiy Score* (Percentage)
40 35 30 25 20 15 10 5 0 1 2 3 1
Session
*Commutative flexibility score = number of modality switches out of the number of opportunities to switch.
Figure 3 Participants Use of Combined Modalities During the RCT Probe across word lists
Baseline 30
Treatment Phase 1
Treatment Phase 2
Post-Treatment
Number of Accurate Combined Productions
25 20 15 10 5 0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 Sessions
Das könnte Ihnen auch gefallen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (894)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Voice Production in Singing and SpeakingBased On Scientific Principles (Fourth Edition, Revised and Enlarged) by Mills, Wesley, 1847-1915Dokument165 SeitenVoice Production in Singing and SpeakingBased On Scientific Principles (Fourth Edition, Revised and Enlarged) by Mills, Wesley, 1847-1915Gutenberg.org100% (3)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- 7 Day Free Guide PDFDokument14 Seiten7 Day Free Guide PDFGuille RodriguezNoch keine Bewertungen
- Revised Market Potential Estimates for Biopure's Hemopure Based on Competitive LandscapeDokument4 SeitenRevised Market Potential Estimates for Biopure's Hemopure Based on Competitive Landscapeargand_xw9097Noch keine Bewertungen
- Ultrasonic Therapy UnitDokument9 SeitenUltrasonic Therapy UnitRiya KumariNoch keine Bewertungen
- Initiatives of FSSAIDokument27 SeitenInitiatives of FSSAIAshok Yadav100% (2)
- Acne and Whey Protein Supplementation Among Bodybuilders PDFDokument4 SeitenAcne and Whey Protein Supplementation Among Bodybuilders PDFHenyta TsuNoch keine Bewertungen
- Kumara Reiki 2013 Attunement NotesDokument17 SeitenKumara Reiki 2013 Attunement NotesHaryadi Yadi100% (2)
- Neonatal Thrombocytopenia: An Overview of Etiologies and ManagementDokument21 SeitenNeonatal Thrombocytopenia: An Overview of Etiologies and ManagementbidisNoch keine Bewertungen
- Clatsop District Attorney Ron Brown Combined Bar Complaints 12-1-23Dokument333 SeitenClatsop District Attorney Ron Brown Combined Bar Complaints 12-1-23mary engNoch keine Bewertungen
- 2023 0203 Original Inquiry BROWN Reyneke Redacted-1Dokument58 Seiten2023 0203 Original Inquiry BROWN Reyneke Redacted-1mary engNoch keine Bewertungen
- Disability Rights Oregon Opposed To Expanded Civil Commitment Law SB 187Dokument2 SeitenDisability Rights Oregon Opposed To Expanded Civil Commitment Law SB 187mary engNoch keine Bewertungen
- Clatsop District Attorney Ron Brown Combined Bar Complaints 12-1-23Dokument333 SeitenClatsop District Attorney Ron Brown Combined Bar Complaints 12-1-23mary engNoch keine Bewertungen
- Brown Ronald 1994 0418 Admonition Letter 93-156 27565-1Dokument1 SeiteBrown Ronald 1994 0418 Admonition Letter 93-156 27565-1mary engNoch keine Bewertungen
- Leach Larry D. DSM CAO 09-10-18 1801325Dokument6 SeitenLeach Larry D. DSM CAO 09-10-18 1801325mary engNoch keine Bewertungen
- Binder 2001756 RedactedDokument56 SeitenBinder 2001756 Redactedmary engNoch keine Bewertungen
- Wilson Mark J. GC 06-10-10 1000346 Redacted-1Dokument518 SeitenWilson Mark J. GC 06-10-10 1000346 Redacted-1mary engNoch keine Bewertungen
- Cloninger Kasey D DSM CAO 06-26-08 RedactedDokument7 SeitenCloninger Kasey D DSM CAO 06-26-08 Redactedmary engNoch keine Bewertungen
- 2022 1003 Original Inquiry BROWN Barbura - 1Dokument15 Seiten2022 1003 Original Inquiry BROWN Barbura - 1mary engNoch keine Bewertungen
- Pickering Josh A. DSM GC 11-26-18 1801227-1Dokument13 SeitenPickering Josh A. DSM GC 11-26-18 1801227-1mary engNoch keine Bewertungen
- Noll Iain T. DSM CAO 09-27-16 1601470Dokument5 SeitenNoll Iain T. DSM CAO 09-27-16 1601470mary engNoch keine Bewertungen
- Noll Iain T. DSM CAO 09-27-16 1601470Dokument5 SeitenNoll Iain T. DSM CAO 09-27-16 1601470mary engNoch keine Bewertungen
- 2023 0203 Original Inquiry BROWN Reyneke Redacted-1Dokument58 Seiten2023 0203 Original Inquiry BROWN Reyneke Redacted-1mary engNoch keine Bewertungen
- Wilson Mark J. GC 06-10-10 1000346 RedactedDokument518 SeitenWilson Mark J. GC 06-10-10 1000346 Redactedmary engNoch keine Bewertungen
- Pickering Josh A. DSM GC 11-26-18 1801227-1Dokument13 SeitenPickering Josh A. DSM GC 11-26-18 1801227-1mary engNoch keine Bewertungen
- Project Veritas Action Fund v. Rollins, Martin v. Rollins, No. 19-1586 (1st Cir. 2020)Dokument72 SeitenProject Veritas Action Fund v. Rollins, Martin v. Rollins, No. 19-1586 (1st Cir. 2020)mary engNoch keine Bewertungen
- 2022 1003 Original Inquiry BROWN Barbura - 1Dokument15 Seiten2022 1003 Original Inquiry BROWN Barbura - 1mary engNoch keine Bewertungen
- Whistleblower Retaliation Clatsop County 23CR23294 Def DocsDokument265 SeitenWhistleblower Retaliation Clatsop County 23CR23294 Def Docsmary engNoch keine Bewertungen
- Project Veritas v. Schmidt Verified Complaint 2020Dokument18 SeitenProject Veritas v. Schmidt Verified Complaint 2020mary engNoch keine Bewertungen
- Oregon Defender Crisis 11-2023 McshaneDokument32 SeitenOregon Defender Crisis 11-2023 Mcshanemary engNoch keine Bewertungen
- Eng Cease and DesistDokument2 SeitenEng Cease and Desistmary engNoch keine Bewertungen
- Bue Andrew Criminal RecordDokument4 SeitenBue Andrew Criminal Recordmary engNoch keine Bewertungen
- Veritas v. SchmidtDokument78 SeitenVeritas v. Schmidtmary engNoch keine Bewertungen
- Mercy Corps Complaint Final 090722 SignedDokument45 SeitenMercy Corps Complaint Final 090722 Signedmary engNoch keine Bewertungen
- BOLI Re LIfeboat Beacon Discrimination PDFDokument2 SeitenBOLI Re LIfeboat Beacon Discrimination PDFmary engNoch keine Bewertungen
- Eng, Steve Miscellaneous Papers 96-040Dokument1 SeiteEng, Steve Miscellaneous Papers 96-040mary engNoch keine Bewertungen
- Osarch Orak Firearms Arrest - A20154105 - RedactedDokument9 SeitenOsarch Orak Firearms Arrest - A20154105 - Redactedmary engNoch keine Bewertungen
- HumanResourceExploitationManual CIA PDFDokument135 SeitenHumanResourceExploitationManual CIA PDFLouis CorreaNoch keine Bewertungen
- STEPHEN SINGER, Plaintiff, vs. THE STATE OF OREGON by and Through The PUBLIC DEFENSE SERVICES COMMISSION, Defendant.Dokument35 SeitenSTEPHEN SINGER, Plaintiff, vs. THE STATE OF OREGON by and Through The PUBLIC DEFENSE SERVICES COMMISSION, Defendant.mary engNoch keine Bewertungen
- Canadian Standards For Hospital LibrariesDokument4 SeitenCanadian Standards For Hospital LibrariesFernando HernandezNoch keine Bewertungen
- Dengulata KosamDokument3 SeitenDengulata KosamChina SaidaNoch keine Bewertungen
- Pharmacovigilance Classification & CodingDokument42 SeitenPharmacovigilance Classification & Codingrakesh meher0% (1)
- Disectie AnatomieDokument908 SeitenDisectie AnatomieMircea SimionNoch keine Bewertungen
- Safe AnalgesicsDokument3 SeitenSafe AnalgesicsJohn SolisNoch keine Bewertungen
- Reverse Optic Capture of The SingleDokument10 SeitenReverse Optic Capture of The SingleIfaamaninaNoch keine Bewertungen
- ProspectusDokument52 SeitenProspectusRabinder BakhshiNoch keine Bewertungen
- Star HealthDokument451 SeitenStar Healthsanjay prasadNoch keine Bewertungen
- Genetic Counseling: A Study and SuggestionsDokument10 SeitenGenetic Counseling: A Study and SuggestionsraphynjNoch keine Bewertungen
- Chapter 16/lecture #9 Histamine and Antihistaminics Dr. TAC Abella July 22, 2014Dokument8 SeitenChapter 16/lecture #9 Histamine and Antihistaminics Dr. TAC Abella July 22, 2014Rose AnnNoch keine Bewertungen
- Symposiumbooklet CareerDokument36 SeitenSymposiumbooklet Careerroh009Noch keine Bewertungen
- Annamalai University Postgraduate Medical Programmes 2020-2021Dokument12 SeitenAnnamalai University Postgraduate Medical Programmes 2020-2021Velmurugan mNoch keine Bewertungen
- Phase 1 Mixed - MCQDokument74 SeitenPhase 1 Mixed - MCQLee June LyngNoch keine Bewertungen
- Poster ROICAM 2018Dokument1 SeitePoster ROICAM 2018ibrahimNoch keine Bewertungen
- Toxic Metabolic Encephalopathy John W. Melton, M.DDokument17 SeitenToxic Metabolic Encephalopathy John W. Melton, M.DabdalkhalidNoch keine Bewertungen
- Massive Haemorrhage: P Donnelly B FergusonDokument18 SeitenMassive Haemorrhage: P Donnelly B FergusonRizqiNoch keine Bewertungen
- Material Safety Data Sheet: Tert-Amyl Alcohol MSDSDokument6 SeitenMaterial Safety Data Sheet: Tert-Amyl Alcohol MSDSmicaziv4786Noch keine Bewertungen
- Low Back Pain in Elderly AgeingDokument29 SeitenLow Back Pain in Elderly AgeingJane ChaterineNoch keine Bewertungen
- General Survey TECHNIQUE Actual Findings Normal Findings AnalysisDokument21 SeitenGeneral Survey TECHNIQUE Actual Findings Normal Findings AnalysisJerry Joseph B. AbordoNoch keine Bewertungen
- ANATOMY AND PHYSIOLOGY of RabiesDokument5 SeitenANATOMY AND PHYSIOLOGY of RabiesDavid CalaloNoch keine Bewertungen
- EMTALADokument5 SeitenEMTALAJimmy MillerNoch keine Bewertungen
- ActivatorDokument69 SeitenActivatorParijat Chakraborty PJNoch keine Bewertungen