Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Social Welfare Administrartion McqsDokument2 SeitenSocial Welfare Administrartion McqsAbd ur Rehman Vlogs & VideosNoch keine Bewertungen
- FreezingDokument59 SeitenFreezingManoj Rathod100% (1)
- Packaged Drinking Water Project ProfileDokument5 SeitenPackaged Drinking Water Project ProfileArpna BhatiaNoch keine Bewertungen
- UK Code of Practice For Tampon Manufactures and DistributorsDokument9 SeitenUK Code of Practice For Tampon Manufactures and DistributorsFuzzy_Wood_PersonNoch keine Bewertungen
- A. Define Infertility: Objectives: Intended Learning Outcomes That TheDokument2 SeitenA. Define Infertility: Objectives: Intended Learning Outcomes That TheJc Mae CuadrilleroNoch keine Bewertungen
- Pharmacology Mock Exam MCQDokument8 SeitenPharmacology Mock Exam MCQanaeshklNoch keine Bewertungen
- IFCC Visiting LectureDokument3 SeitenIFCC Visiting LectureMaruhum NurNoch keine Bewertungen
- Isolation and Identification of Bacteria ThesisDokument7 SeitenIsolation and Identification of Bacteria Thesisafbtbegxe100% (2)
- SITXWHS001 Assessment 1 (4) Incident ReportDokument7 SeitenSITXWHS001 Assessment 1 (4) Incident Reportpra Deep100% (1)
- Perioperative NursingDokument8 SeitenPerioperative NursingGil Platon Soriano100% (3)
- MicroMaxx 3.3 UG ENG P06435-02B e 1 - 1Dokument200 SeitenMicroMaxx 3.3 UG ENG P06435-02B e 1 - 1Waheed MidoNoch keine Bewertungen
- Dental Restorative Digital Workflow: Digital Smile Design From Aesthetic To Function PDFDokument12 SeitenDental Restorative Digital Workflow: Digital Smile Design From Aesthetic To Function PDFCamilo GuerreroNoch keine Bewertungen
- 32 Vol4 EpaperDokument32 Seiten32 Vol4 EpaperThesouthasian TimesNoch keine Bewertungen
- Qatar Healthcare Facilities Contact GuideDokument3 SeitenQatar Healthcare Facilities Contact GuideShibu KavullathilNoch keine Bewertungen
- Scoring BPSDDokument4 SeitenScoring BPSDayu yuliantiNoch keine Bewertungen
- Prevalence of Pneumonia and Factors Associated Among Children 259 Months Old in Wondo Genet District Sidama Zone SNNPR Ethiopia - PDDokument7 SeitenPrevalence of Pneumonia and Factors Associated Among Children 259 Months Old in Wondo Genet District Sidama Zone SNNPR Ethiopia - PDMusainah FeisalNoch keine Bewertungen
- Management of Class I Type 3 Malocclusion Using Simple Removable AppliancesDokument5 SeitenManagement of Class I Type 3 Malocclusion Using Simple Removable AppliancesMuthia DewiNoch keine Bewertungen
- Earth Leakage Testing Report: Panel Name: Testing Device: Rccb (Iδn) : 30 MaDokument1 SeiteEarth Leakage Testing Report: Panel Name: Testing Device: Rccb (Iδn) : 30 MaAmjad AlbahtiNoch keine Bewertungen
- MalariaDokument11 SeitenMalariaWynli Fullo AncogNoch keine Bewertungen
- OCPD: Symptoms, Diagnosis and TreatmentDokument4 SeitenOCPD: Symptoms, Diagnosis and TreatmentRana Muhammad Ahmad Khan ManjNoch keine Bewertungen
- 'No Evidence That CT Scans, X-Rays Cause Cancer' - Medical News TodayDokument3 Seiten'No Evidence That CT Scans, X-Rays Cause Cancer' - Medical News TodayDr-Aditya ChauhanNoch keine Bewertungen
- Influence of Social Capital On HealthDokument11 SeitenInfluence of Social Capital On HealthHobi's Important BusinesseuNoch keine Bewertungen
- "PASS" Principles For Predictable PDFDokument10 Seiten"PASS" Principles For Predictable PDFkishan bordaNoch keine Bewertungen
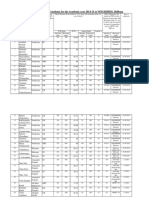
- Admission For 1st Year MBBS Students For The Academic Year 2014-2015Dokument10 SeitenAdmission For 1st Year MBBS Students For The Academic Year 2014-2015Guma KipaNoch keine Bewertungen
- As 2550.5-2002 Cranes Hoists and Winches - Safe Use Mobile CranesDokument8 SeitenAs 2550.5-2002 Cranes Hoists and Winches - Safe Use Mobile CranesSAI Global - APACNoch keine Bewertungen
- Food Production (409) : Sample Question Paper Class X (2018-19) (NSQF)Dokument2 SeitenFood Production (409) : Sample Question Paper Class X (2018-19) (NSQF)Janavi M SNoch keine Bewertungen
- Chapter 22 The First Heart SoundDokument5 SeitenChapter 22 The First Heart SoundAbhilash ReddyNoch keine Bewertungen
- Facts of MaintenanceDokument9 SeitenFacts of Maintenancegeorge youssefNoch keine Bewertungen
- CG A022 01 Shortened Dental ArchDokument5 SeitenCG A022 01 Shortened Dental ArchmahmoudNoch keine Bewertungen
- Case Report: Communication Strategies For Empowering and Protecting ChildrenDokument9 SeitenCase Report: Communication Strategies For Empowering and Protecting ChildrennabilahNoch keine Bewertungen