Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The Role of Self-Compassion in Romantic RelationshipsDokument22 SeitenThe Role of Self-Compassion in Romantic Relationshipshenry4chinaski100% (1)
- Career Calling Lecture - Dylan FirsickDokument3 SeitenCareer Calling Lecture - Dylan Firsickhenry4chinaskiNoch keine Bewertungen
- The Role of Self-Compassion in Romantic RelationshipsDokument22 SeitenThe Role of Self-Compassion in Romantic Relationshipshenry4chinaski100% (1)
- COPS LquestionnaireDokument2 SeitenCOPS Lquestionnairehenry4chinaskiNoch keine Bewertungen
- The Campbell Interest and Skill Survey (CISS) : A Product of Ninety Years of Psychometric Evolution Journal of Career Assessment 1995 Campbell 391 410Dokument21 SeitenThe Campbell Interest and Skill Survey (CISS) : A Product of Ninety Years of Psychometric Evolution Journal of Career Assessment 1995 Campbell 391 410henry4chinaskiNoch keine Bewertungen
- Eating Disorders and Diabetes PDFDokument4 SeitenEating Disorders and Diabetes PDFhenry4chinaskiNoch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Diet, Insulin and Blood Glucose: © Food - A Fact of Life 2009Dokument22 SeitenDiet, Insulin and Blood Glucose: © Food - A Fact of Life 2009Eliana MuisNoch keine Bewertungen
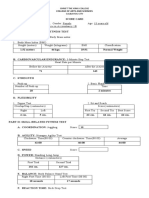
- Physical Fitness Test Score CardDokument2 SeitenPhysical Fitness Test Score CardDivine Cardejon50% (4)
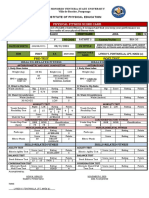
- Pre-Test Post Test: Physical Fitness Score CardDokument2 SeitenPre-Test Post Test: Physical Fitness Score CardRed CactusNoch keine Bewertungen
- Integrated EnglishDokument158 SeitenIntegrated EnglishRachel Ria Felisiana sidebangNoch keine Bewertungen
- Body Mass Index WorksheetDokument2 SeitenBody Mass Index WorksheetYasser EidNoch keine Bewertungen
- Ji 2019Dokument10 SeitenJi 2019Igor SousaNoch keine Bewertungen
- Department of Education School Form 8 Learner's Basic Health and Nutrition Report (SF8)Dokument2 SeitenDepartment of Education School Form 8 Learner's Basic Health and Nutrition Report (SF8)Maria Cristina DelmoNoch keine Bewertungen
- Project HFDokument136 SeitenProject HFCutiee 49Noch keine Bewertungen
- Chapter - 6 Test and MeasurementDokument11 SeitenChapter - 6 Test and MeasurementLakshaya YadavNoch keine Bewertungen
- Failure To Thrive - AAPDokument11 SeitenFailure To Thrive - AAPAlexNoch keine Bewertungen
- SF 8Dokument12 SeitenSF 8Crisadel Largo AlferezNoch keine Bewertungen
- Calories Needed For A 16 Year Old, 66 KG FemaleDokument1 SeiteCalories Needed For A 16 Year Old, 66 KG FemaleViktoria SaerangNoch keine Bewertungen
- Role ModelDokument61 SeitenRole ModelGuru HegdeNoch keine Bewertungen
- Calories Needed For A 19 Year Old, 59 KG FemaleDokument7 SeitenCalories Needed For A 19 Year Old, 59 KG FemaleMutiarahmawati MootaluNoch keine Bewertungen
- Lesson 4Dokument8 SeitenLesson 4Sheena Mae Po100% (1)
- Soalan Assignment Stm10173Dokument7 SeitenSoalan Assignment Stm10173Razanah RozaimayNoch keine Bewertungen
- Nursing Care PlanDokument11 SeitenNursing Care PlanKevin John ReaLubit SaLisi100% (6)
- HOPE1 - q1 - Mod 1Dokument30 SeitenHOPE1 - q1 - Mod 1Julie Anne Tolentino83% (6)
- Lecture 8 VBADokument10 SeitenLecture 8 VBAJonahJuniorNoch keine Bewertungen
- Food and Nutrition VocabularyDokument2 SeitenFood and Nutrition Vocabularyedward100% (1)
- To Lose Weight The Wrong Way Is A Health FactorDokument12 SeitenTo Lose Weight The Wrong Way Is A Health FactorBernard EasterlingNoch keine Bewertungen
- Acute Inflammatory Edema: A Mimicker of Cellulitis in Critically Ill PatientsDokument6 SeitenAcute Inflammatory Edema: A Mimicker of Cellulitis in Critically Ill PatientsibrahimNoch keine Bewertungen
- Fitness RX For Women - April 2014Dokument116 SeitenFitness RX For Women - April 2014Ricardo Soares100% (2)
- 2019 Nutrition in Cystic Fibrosis - From The Past To The Present and Into The FutureDokument18 Seiten2019 Nutrition in Cystic Fibrosis - From The Past To The Present and Into The FutureMaria Paula CastroNoch keine Bewertungen
- LE Gr4 PEandHealth Q1 V3.-Week4 FINAL-erniferDokument15 SeitenLE Gr4 PEandHealth Q1 V3.-Week4 FINAL-erniferJulie Ann EsparagozaNoch keine Bewertungen
- Obese Filipinos Now Ballooning: Henrylito D. TacioDokument6 SeitenObese Filipinos Now Ballooning: Henrylito D. TacioAmara NnannaNoch keine Bewertungen
- Appetite: Ester F.C. Sleddens, Stef P.J. Kremers, Nanne K. de Vries, Carel ThijsDokument3 SeitenAppetite: Ester F.C. Sleddens, Stef P.J. Kremers, Nanne K. de Vries, Carel ThijsNancy Veronica HutajuluNoch keine Bewertungen
- The Importance of Evaluating The Impact of Continuing Nursing Education September 2014Dokument10 SeitenThe Importance of Evaluating The Impact of Continuing Nursing Education September 2014Jairus Joel A. SuminegNoch keine Bewertungen
- Bioelectrical Impedance Analysis (BIA) and Phase Angle PDFDokument16 SeitenBioelectrical Impedance Analysis (BIA) and Phase Angle PDFiomastNoch keine Bewertungen
- UnitVII-2Nutrition and DietDokument38 SeitenUnitVII-2Nutrition and DietYuNa YoshinoyaNoch keine Bewertungen