Das könnte Ihnen auch gefallen
- Jurnal Kedok 5Dokument4 SeitenJurnal Kedok 5Adill HusadaNoch keine Bewertungen
- Artikel 1 - American Medical Education 100 YearsDokument15 SeitenArtikel 1 - American Medical Education 100 YearsAdill HusadaNoch keine Bewertungen
- Alpro 2Dokument1 SeiteAlpro 2Adill HusadaNoch keine Bewertungen
- Alpro 2Dokument1 SeiteAlpro 2Adill HusadaNoch keine Bewertungen
- Alpro 2Dokument1 SeiteAlpro 2Adill HusadaNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Application For Schengen Visa: This Application Form Is FreeDokument2 SeitenApplication For Schengen Visa: This Application Form Is FreeMonirul IslamNoch keine Bewertungen
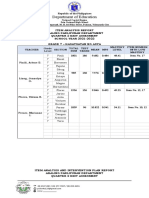
- Item Analysis Repost Sy2022Dokument4 SeitenItem Analysis Repost Sy2022mjeduriaNoch keine Bewertungen
- Labour Laws Individual Assignment - Code On Wages Subject Code: MHR4CCHR05Dokument5 SeitenLabour Laws Individual Assignment - Code On Wages Subject Code: MHR4CCHR05Seher BhatiaNoch keine Bewertungen
- Blaw 1000 ReviewerDokument10 SeitenBlaw 1000 ReviewerKyla FacunlaNoch keine Bewertungen
- AD&D Crime and PunishmentDokument10 SeitenAD&D Crime and PunishmentI_NiemandNoch keine Bewertungen
- STAMPF V TRIGG - OpinionDokument32 SeitenSTAMPF V TRIGG - Opinionml07751Noch keine Bewertungen
- 4IS1 - 01 - Que - 20210504 QP 2021Dokument28 Seiten4IS1 - 01 - Que - 20210504 QP 2021fmunazza146Noch keine Bewertungen
- What Is Leave Travel Allowance or LTADokument3 SeitenWhat Is Leave Travel Allowance or LTAMukesh UpadhyeNoch keine Bewertungen
- (7-3) Meco Manning vs. CuyosDokument7 Seiten(7-3) Meco Manning vs. CuyosJan Carlo SanchezNoch keine Bewertungen
- Pay rates for Miscellaneous Award 2010Dokument8 SeitenPay rates for Miscellaneous Award 2010JoshNoch keine Bewertungen
- CW: Union Victory at Gettysburg & VicksburgDokument9 SeitenCW: Union Victory at Gettysburg & VicksburgPi LoverNoch keine Bewertungen
- Swot Analysis of IB in PakistanDokument2 SeitenSwot Analysis of IB in PakistanMubeen Zubair100% (2)
- TL01 Behold Terra LibraDokument15 SeitenTL01 Behold Terra LibraKeyProphet100% (1)
- Criminal Law 1 NotesDokument3 SeitenCriminal Law 1 Notesmbdometita100% (1)
- Black SupremacistDokument7 SeitenBlack SupremacistJoMarie13Noch keine Bewertungen
- Install Bucket ElevatorsDokument77 SeitenInstall Bucket ElevatorsYhaneNoch keine Bewertungen
- Paper On Society1 Modernity PDFDokument13 SeitenPaper On Society1 Modernity PDFferiha goharNoch keine Bewertungen
- The Magnificent-Equity ValuationDokument70 SeitenThe Magnificent-Equity ValuationMohit TewaryNoch keine Bewertungen
- Marking Guide for Contract Administration ExamDokument7 SeitenMarking Guide for Contract Administration Examრაქსშ საჰაNoch keine Bewertungen
- Question 3-FSDokument1 SeiteQuestion 3-FSRax-Nguajandja KapuireNoch keine Bewertungen
- Combination Resume SampleDokument2 SeitenCombination Resume SampleDavid SavelaNoch keine Bewertungen
- ACCT5001 2022 S2 - Module 3 - Lecture Slides StudentDokument33 SeitenACCT5001 2022 S2 - Module 3 - Lecture Slides Studentwuzhen102110Noch keine Bewertungen
- Legal Ethics Oral Examination 2018Dokument13 SeitenLegal Ethics Oral Examination 2018Telle MarieNoch keine Bewertungen
- WT ADMIT CARD STEPSDokument1 SeiteWT ADMIT CARD STEPSSonam ShahNoch keine Bewertungen
- F2800-11 Standard Specification For Recirculating Hood System For Cooking AppliancesDokument4 SeitenF2800-11 Standard Specification For Recirculating Hood System For Cooking AppliancesjohnnyNoch keine Bewertungen
- All CCDokument7 SeitenAll CCpabloespinosapiedras23100% (1)
- To Sell or Scale Up: Canada's Patent Strategy in A Knowledge EconomyDokument22 SeitenTo Sell or Scale Up: Canada's Patent Strategy in A Knowledge EconomyInstitute for Research on Public Policy (IRPP)Noch keine Bewertungen
- Unit 1-5Dokument122 SeitenUnit 1-5STUTI RAJNoch keine Bewertungen
- QO-D-7.1-3 Ver-4.0 - Withdrawal of Specification of ItemsDokument3 SeitenQO-D-7.1-3 Ver-4.0 - Withdrawal of Specification of ItemsSaugata HalderNoch keine Bewertungen
- Licensing AgreementDokument9 SeitenLicensing AgreementberrolawfirmNoch keine Bewertungen