Das könnte Ihnen auch gefallen
- Master Lesson PlanDokument8 SeitenMaster Lesson Planapi-253396474Noch keine Bewertungen
- Northern Ballet Theatre Academy - 2010 BrochureDokument16 SeitenNorthern Ballet Theatre Academy - 2010 BrochureNorthern BalletNoch keine Bewertungen
- Ballet TerminologyDokument2 SeitenBallet TerminologykeipenceNoch keine Bewertungen
- Unit 43 Developing Classical Ballet TechniqueDokument11 SeitenUnit 43 Developing Classical Ballet Techniquebernicetsy100% (1)
- Labanotation Movement LanguageDokument11 SeitenLabanotation Movement Languageplavi zecNoch keine Bewertungen
- Ballet PageDokument1 SeiteBallet Pagemcorrea5527Noch keine Bewertungen
- What Is Neoclassical BalletDokument2 SeitenWhat Is Neoclassical BalletAlice Chacon100% (1)
- Ohad NaharinDokument15 SeitenOhad NaharinmartinaNoch keine Bewertungen
- Ballet Recovery and Blister FixingDokument12 SeitenBallet Recovery and Blister FixingMichael GillanNoch keine Bewertungen
- Dancers DozenDokument20 SeitenDancers DozenCandice Maxie DingDingNoch keine Bewertungen
- Ways To Teach Dance ToDokument4 SeitenWays To Teach Dance Toapi-302265057Noch keine Bewertungen
- Teaching The Dance Class StrategiesDokument8 SeitenTeaching The Dance Class StrategieshugoNoch keine Bewertungen
- Modern Jazz DanceDokument14 SeitenModern Jazz DanceAlFrancisCayagaNoch keine Bewertungen
- Modern Theatre Syllabus Outline 2015 RevDokument46 SeitenModern Theatre Syllabus Outline 2015 RevSayo TakanashitoNoch keine Bewertungen
- Basic Terms of BalletDokument5 SeitenBasic Terms of BalletHocheerNoch keine Bewertungen
- Cecchetti Theory Grade Advanced1Dokument7 SeitenCecchetti Theory Grade Advanced1kikkina_91100% (1)
- Ballet Study Guide ATRUDokument12 SeitenBallet Study Guide ATRUKarla Zavala Robles100% (1)
- The Art of ChoreographyDokument22 SeitenThe Art of ChoreographyRosa Meneses100% (2)
- TPPS Manual EbookDokument129 SeitenTPPS Manual EbookInês de CastroNoch keine Bewertungen
- Turnout For Dancers: Hip Anatomy and Factors Affecting TurnoutDokument7 SeitenTurnout For Dancers: Hip Anatomy and Factors Affecting TurnoutsstavrosNoch keine Bewertungen
- Grade 5Dokument27 SeitenGrade 5api-450701173Noch keine Bewertungen
- 201602109EIRR FinalDokument56 Seiten201602109EIRR FinaltomimitoNoch keine Bewertungen
- Mr. GagaDokument7 SeitenMr. GagaPaige HollingsworthNoch keine Bewertungen
- JBS Trainee HandbookDokument19 SeitenJBS Trainee HandbookAxel GalindoNoch keine Bewertungen
- Ballet For BabiesDokument6 SeitenBallet For BabiesTGCD1Noch keine Bewertungen
- Classical Ballet Syllabus Grade 6: Level 3 Award in Graded Examinations in Dance Female SyllabusDokument54 SeitenClassical Ballet Syllabus Grade 6: Level 3 Award in Graded Examinations in Dance Female SyllabusMara Meira DavidNoch keine Bewertungen
- Ballet One Ballet Class SyllabusDokument3 SeitenBallet One Ballet Class SyllabusEliza MarieNoch keine Bewertungen
- Dance and Improvisation PHD Thesis PDFDokument320 SeitenDance and Improvisation PHD Thesis PDFAnonymous CjcDVK54Noch keine Bewertungen
- Beginning PointeDokument10 SeitenBeginning PointeSimona Lakklisa50% (2)
- Modern DanceDokument20 SeitenModern DanceHannah AlvarezNoch keine Bewertungen
- Dance Choreography RulesDokument1 SeiteDance Choreography Rulesapi-377964292Noch keine Bewertungen
- Cecchetti Syllabus OutllineDokument75 SeitenCecchetti Syllabus OutllineTaylor Bradford80% (5)
- In Pursuit of The SylphDokument23 SeitenIn Pursuit of The SylphKimora Brock100% (1)
- Bales & Eliot - Dance On Its Own TermsDokument455 SeitenBales & Eliot - Dance On Its Own TermsManuel CoitoNoch keine Bewertungen
- 1imperial Classical Ballet Syllabus OutlineDokument91 Seiten1imperial Classical Ballet Syllabus Outlinebernicetsy100% (2)
- National Ballet-STUDY GUIDE, Dance AboutDokument16 SeitenNational Ballet-STUDY GUIDE, Dance AboutAnonymous SmtsMiad100% (1)
- Ballet Vocab ChartDokument6 SeitenBallet Vocab ChartAnonymous q6G7K1wNoch keine Bewertungen
- Ballet Lesson PlanDokument3 SeitenBallet Lesson PlanKate HartmannNoch keine Bewertungen
- Dance 460 Ballet Research PaperDokument10 SeitenDance 460 Ballet Research Papercalius1Noch keine Bewertungen
- Collection of Classical Ballet VariationsDokument51 SeitenCollection of Classical Ballet VariationsSarah Kim100% (1)
- Tanztechniken 2010 PDFDokument304 SeitenTanztechniken 2010 PDFAngelina Georgieva100% (1)
- Principles of ChoreographyDokument1 SeitePrinciples of ChoreographyOhiwei OsawemenNoch keine Bewertungen
- Cuban Ballet 134-164Dokument30 SeitenCuban Ballet 134-164Daniel Bellas100% (2)
- Vera Kostrovitskaya 100 Lessons in Classical BalletDokument26 SeitenVera Kostrovitskaya 100 Lessons in Classical BalletGisela Ferreira50% (8)
- Classical Ballet DanceDokument31 SeitenClassical Ballet DanceJay CeeNoch keine Bewertungen
- 2oth Century Modern DanceDokument41 Seiten2oth Century Modern DanceNATHANIEL CORTEZNoch keine Bewertungen
- Musical Theatre Heritage Reading ListDokument4 SeitenMusical Theatre Heritage Reading ListAris Nur AzharNoch keine Bewertungen
- Essential Dance MedicineDokument184 SeitenEssential Dance MedicineRobert Von Richthofen92% (12)
- Third Swan from the Left: The Stories, Musings, and Random Thoughts of a Wandering ArtistVon EverandThird Swan from the Left: The Stories, Musings, and Random Thoughts of a Wandering ArtistNoch keine Bewertungen
- Classical Ballet2 1Dokument71 SeitenClassical Ballet2 1DeSouza Juvita100% (1)
- Ballet Syllabus in Its Entirety - 2017 - 2018Dokument26 SeitenBallet Syllabus in Its Entirety - 2017 - 2018Mihaela Mihis100% (1)
- Suzanne K. Walther-The Dance Theatre - Kurt Jooss (Choreography and Dance) (1997)Dokument104 SeitenSuzanne K. Walther-The Dance Theatre - Kurt Jooss (Choreography and Dance) (1997)Weronique100% (1)
- Maya Plisetskaya's Groundbreaking Career as a Soviet BallerinaDokument10 SeitenMaya Plisetskaya's Groundbreaking Career as a Soviet BallerinaAnonymous J5vpGuNoch keine Bewertungen
- KPOP DanceDokument1 SeiteKPOP DanceJairo TanyagNoch keine Bewertungen
- NDW Grades 5 8 Modern Dance Lesson Plans1Dokument20 SeitenNDW Grades 5 8 Modern Dance Lesson Plans1Joe LevinneNoch keine Bewertungen
- Teaching Methods Ballet 1 ClassDokument10 SeitenTeaching Methods Ballet 1 ClassNicoleMakenaBrowneNoch keine Bewertungen
- History of Contemporary Jazz (Seni Tari)Dokument2 SeitenHistory of Contemporary Jazz (Seni Tari)Rainy SiiNoch keine Bewertungen
- Modern Bodies: Dance and American Modernism from Martha Graham to Alvin AileyVon EverandModern Bodies: Dance and American Modernism from Martha Graham to Alvin AileyNoch keine Bewertungen
- Basic BalletDokument3 SeitenBasic BalletMarco Torres100% (2)
- The Physiology OF BloodDokument41 SeitenThe Physiology OF Bloodpop67Noch keine Bewertungen
- Problems of The Ballet DancerDokument6 SeitenProblems of The Ballet Dancerpop67Noch keine Bewertungen
- Musculoskeletal InjuriesDokument5 SeitenMusculoskeletal Injuriespop67Noch keine Bewertungen
- Performance StressDokument5 SeitenPerformance Stresspop67Noch keine Bewertungen
- Taking Class Memoirs of A Classroom BallerinaDokument15 SeitenTaking Class Memoirs of A Classroom Ballerinapop67Noch keine Bewertungen
- DaytodayDokument6 SeitenDaytodaypop67Noch keine Bewertungen
- Sociological ReviewDokument17 SeitenSociological Reviewpop67Noch keine Bewertungen
- Ucalgary 2012 Mcewen KristaDokument160 SeitenUcalgary 2012 Mcewen Kristapop67Noch keine Bewertungen
- Foundationsforexcellence2009 1Dokument72 SeitenFoundationsforexcellence2009 1pop67Noch keine Bewertungen
- Musculoskeletal InjuriesDokument5 SeitenMusculoskeletal Injuriespop67Noch keine Bewertungen
- BMJ 3310594 BDokument2 SeitenBMJ 3310594 Bpop67Noch keine Bewertungen
- Bulletin For Teachers 2-1 Pp5-8 McCormackDokument4 SeitenBulletin For Teachers 2-1 Pp5-8 McCormackpop67Noch keine Bewertungen
- The Signficance of RespirationDokument12 SeitenThe Signficance of RespirationApril Dawn100% (1)
- BMJ 3310594 BDokument2 SeitenBMJ 3310594 Bpop67Noch keine Bewertungen
- Between Scylla and Charybdis. Nutritional Education Versus Body Culture and The Ballet Aesthetic The Effects On The Lives of Female DancersDokument18 SeitenBetween Scylla and Charybdis. Nutritional Education Versus Body Culture and The Ballet Aesthetic The Effects On The Lives of Female Dancerspop67Noch keine Bewertungen
- Maternal Diet and Gestational Factors Linked to Boys' Hypospadias RiskDokument6 SeitenMaternal Diet and Gestational Factors Linked to Boys' Hypospadias Riskpldhy2004Noch keine Bewertungen
- Injury and Joint HypermobilityDokument2 SeitenInjury and Joint Hypermobilitypop67Noch keine Bewertungen
- Motor Control TheoriesDokument94 SeitenMotor Control Theoriespop67Noch keine Bewertungen
- Motor Control TheoriesDokument94 SeitenMotor Control Theoriespop67Noch keine Bewertungen
- Merritt Morning Market 2747 - July 13Dokument2 SeitenMerritt Morning Market 2747 - July 13Kim LeclairNoch keine Bewertungen
- Grade 9 Waltz WorksheetDokument6 SeitenGrade 9 Waltz WorksheetWilmar EspinosaNoch keine Bewertungen
- Hobbies VocabularyDokument6 SeitenHobbies VocabularyCamilo Caicedo GNoch keine Bewertungen
- Physical Activities in The Philippines During The Pre-Spanish PeriodDokument2 SeitenPhysical Activities in The Philippines During The Pre-Spanish PeriodNa AbdurahimNoch keine Bewertungen
- Laduma: Soccer, Politics and Society in South Africa, From Its Origins To 2010Dokument17 SeitenLaduma: Soccer, Politics and Society in South Africa, From Its Origins To 2010LittleWhiteBakkie0% (1)
- Unit 1 - Families: Discover English Starter PHOTOCOPIABLE © PearsonDokument8 SeitenUnit 1 - Families: Discover English Starter PHOTOCOPIABLE © PearsonOmar MokhtarNoch keine Bewertungen
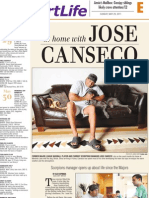
- "At Home With Jose Canseco" LayoutDokument2 Seiten"At Home With Jose Canseco" LayoutNatalie DeBruinNoch keine Bewertungen
- Special TestDokument12 SeitenSpecial TestSIMPLEJGNoch keine Bewertungen
- Dancesport LetterDokument3 SeitenDancesport Letterivy macalaladNoch keine Bewertungen
- Annual Book 2009Dokument80 SeitenAnnual Book 2009Chirag.B. VaghelaNoch keine Bewertungen
- Great Gatsby ScriptDokument133 SeitenGreat Gatsby ScriptSatyani Adiwibowo100% (1)
- Chris Cool TEEN Agent Sereis #5 Heads You LoseDokument175 SeitenChris Cool TEEN Agent Sereis #5 Heads You LosePastPresentFuture100% (1)
- Paso Doble ASHGODokument7 SeitenPaso Doble ASHGOFranz Anthony Quirit GoNoch keine Bewertungen
- Tampines News Aug Sep 08Dokument12 SeitenTampines News Aug Sep 08Tampines Town0% (1)
- Different Ways To Look at Flamenco PalosDokument28 SeitenDifferent Ways To Look at Flamenco PalosPablo_SPMNoch keine Bewertungen
- Physical Education and Health 3: Nature and Background of The Different DancesDokument22 SeitenPhysical Education and Health 3: Nature and Background of The Different Dancesseph bronNoch keine Bewertungen
- Reported Speech EjerciciosDokument6 SeitenReported Speech EjerciciosLaura BrazaNoch keine Bewertungen
- December 19, 2014Dokument36 SeitenDecember 19, 2014Anonymous KMKk9Msn5Noch keine Bewertungen
- Gurdjieff-Oriental Suite TracklistDokument4 SeitenGurdjieff-Oriental Suite TracklisttammozNoch keine Bewertungen
- Polish DanceDokument4 SeitenPolish DanceKen PfrengerNoch keine Bewertungen
- New Zealand AnglDokument6 SeitenNew Zealand AnglIuliaNoch keine Bewertungen
- Pe and HealthDokument29 SeitenPe and Healthvan dulayNoch keine Bewertungen
- Lansing Fish Days 2014Dokument8 SeitenLansing Fish Days 2014The Standard NewspaperNoch keine Bewertungen
- Ursula PughDokument6 SeitenUrsula PughFaysal JemaiNoch keine Bewertungen
- Ceilidh MusicDokument42 SeitenCeilidh Musicasdf_asdf196175% (4)
- The History of The Appearance and Development of DancesportDokument19 SeitenThe History of The Appearance and Development of DancesportAndreea CodreanuNoch keine Bewertungen
- Social and Ballroom Dances LectureDokument3 SeitenSocial and Ballroom Dances LectureGlaiza Escosia Ager100% (1)
- Rank YB Time PTS: Points: FINA 2021Dokument19 SeitenRank YB Time PTS: Points: FINA 2021KarolisNoch keine Bewertungen
- Street DanceDokument7 SeitenStreet DanceJhay LongakitNoch keine Bewertungen
- This Course Will Provide Students With Basic Knowledge in Ballroom DanceDokument2 SeitenThis Course Will Provide Students With Basic Knowledge in Ballroom DanceJohn Jill T. VillamorNoch keine Bewertungen