Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- 6th Central Pay Commission Salary CalculatorDokument15 Seiten6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDokument15 Seiten6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- Special Topics in Income TaxationDokument78 SeitenSpecial Topics in Income TaxationPantas DiwaNoch keine Bewertungen
- 2 - Site Crisis Management Plan TemplateDokument42 Seiten2 - Site Crisis Management Plan Templatesentryx1100% (7)
- Department of Labor: Yr English GuideDokument1 SeiteDepartment of Labor: Yr English GuideUSA_DepartmentOfLaborNoch keine Bewertungen
- Department of Labor: Generalprovision 6 28 07Dokument6 SeitenDepartment of Labor: Generalprovision 6 28 07USA_DepartmentOfLaborNoch keine Bewertungen
- Department of Labor: Dst-Aces-Cps-V20040123Dokument121 SeitenDepartment of Labor: Dst-Aces-Cps-V20040123USA_DepartmentOfLaborNoch keine Bewertungen
- Department of Labor: Aces CPDokument36 SeitenDepartment of Labor: Aces CPUSA_DepartmentOfLabor100% (2)
- Department of Labor: Dst-Aces-Cps-V20040617Dokument121 SeitenDepartment of Labor: Dst-Aces-Cps-V20040617USA_DepartmentOfLaborNoch keine Bewertungen
- Department of Labor: ForkliftstickerDokument1 SeiteDepartment of Labor: ForkliftstickerUSA_DepartmentOfLaborNoch keine Bewertungen
- Department of Labor: Stop2stickerDokument1 SeiteDepartment of Labor: Stop2stickerUSA_DepartmentOfLaborNoch keine Bewertungen
- Department of Labor: YouthworkerDokument1 SeiteDepartment of Labor: YouthworkerUSA_DepartmentOfLaborNoch keine Bewertungen
- Department of Labor: Stop1stickerDokument1 SeiteDepartment of Labor: Stop1stickerUSA_DepartmentOfLaborNoch keine Bewertungen
- Department of Labor: Stop1sticker6Dokument1 SeiteDepartment of Labor: Stop1sticker6USA_DepartmentOfLaborNoch keine Bewertungen
- Department of Labor: JYMP 8x11 3Dokument1 SeiteDepartment of Labor: JYMP 8x11 3USA_DepartmentOfLaborNoch keine Bewertungen
- Department of Labor: Stop2sticker6Dokument1 SeiteDepartment of Labor: Stop2sticker6USA_DepartmentOfLaborNoch keine Bewertungen
- Department of Labor: Forkliftsticker6Dokument1 SeiteDepartment of Labor: Forkliftsticker6USA_DepartmentOfLaborNoch keine Bewertungen
- Department of Labor: LindseyDokument1 SeiteDepartment of Labor: LindseyUSA_DepartmentOfLaborNoch keine Bewertungen
- Department of Labor: YouthRulesBrochureDokument12 SeitenDepartment of Labor: YouthRulesBrochureUSA_DepartmentOfLaborNoch keine Bewertungen
- Department of Labor: 20040422 YouthrulesDokument1 SeiteDepartment of Labor: 20040422 YouthrulesUSA_DepartmentOfLaborNoch keine Bewertungen
- Department of Labor: Niosh Letter FinalDokument3 SeitenDepartment of Labor: Niosh Letter FinalUSA_DepartmentOfLaborNoch keine Bewertungen
- Department of Labor: Niosh Recs To Dol 050302Dokument198 SeitenDepartment of Labor: Niosh Recs To Dol 050302USA_DepartmentOfLaborNoch keine Bewertungen
- Department of Labor: KonstaDokument1 SeiteDepartment of Labor: KonstaUSA_DepartmentOfLaborNoch keine Bewertungen
- Department of Labor: YouthConstructDokument1 SeiteDepartment of Labor: YouthConstructUSA_DepartmentOfLaborNoch keine Bewertungen
- Department of Labor: Final ReportDokument37 SeitenDepartment of Labor: Final ReportUSA_DepartmentOfLaborNoch keine Bewertungen
- Department of Labor: BookmarkDokument2 SeitenDepartment of Labor: BookmarkUSA_DepartmentOfLaborNoch keine Bewertungen
- Department of Labor: ln61003Dokument2 SeitenDepartment of Labor: ln61003USA_DepartmentOfLaborNoch keine Bewertungen
- Department of Labor: JYMP 8x11 1Dokument1 SeiteDepartment of Labor: JYMP 8x11 1USA_DepartmentOfLaborNoch keine Bewertungen
- Department of Labor: JYMP 8x11 2Dokument1 SeiteDepartment of Labor: JYMP 8x11 2USA_DepartmentOfLaborNoch keine Bewertungen
- Department of Labor: JYMP 11x17 1Dokument1 SeiteDepartment of Labor: JYMP 11x17 1USA_DepartmentOfLaborNoch keine Bewertungen
- Department of Labor: JYMP 11x17 3Dokument1 SeiteDepartment of Labor: JYMP 11x17 3USA_DepartmentOfLaborNoch keine Bewertungen
- Department of Labor: JYMP 11x17 2Dokument1 SeiteDepartment of Labor: JYMP 11x17 2USA_DepartmentOfLaborNoch keine Bewertungen
- Legal and Illegal Earning in The Light of Quran and HadithDokument12 SeitenLegal and Illegal Earning in The Light of Quran and HadithComm SofianNoch keine Bewertungen
- QCP Installation of Ahu FahuDokument7 SeitenQCP Installation of Ahu FahuThulani DlaminiNoch keine Bewertungen
- Florentino V SupervalueDokument2 SeitenFlorentino V SupervalueVener Angelo MargalloNoch keine Bewertungen
- Hydro Resources Contractors Corp V Pagalilauan G.R. No. L-62909Dokument3 SeitenHydro Resources Contractors Corp V Pagalilauan G.R. No. L-62909fgNoch keine Bewertungen
- Last Two Verse of Surah AlDokument5 SeitenLast Two Verse of Surah AlMhonly MamangcaoNoch keine Bewertungen
- Notes On Qawaid FiqhiyaDokument2 SeitenNotes On Qawaid FiqhiyatariqsoasNoch keine Bewertungen
- GR No. 186417 People vs. Felipe MirandillaDokument1 SeiteGR No. 186417 People vs. Felipe MirandillaNadine GabaoNoch keine Bewertungen
- Listing of Internet Slang and AcronymsDokument4 SeitenListing of Internet Slang and AcronymsabeegameNoch keine Bewertungen
- Complaint LettersDokument3 SeitenComplaint LettersPriyankkaa BRNoch keine Bewertungen
- InstitutionalismDokument15 SeitenInstitutionalismLowel DalisayNoch keine Bewertungen
- Business Ethics Session 5Dokument9 SeitenBusiness Ethics Session 5EliaQazilbashNoch keine Bewertungen
- 2021 TaxReturnDokument11 Seiten2021 TaxReturnHa AlNoch keine Bewertungen
- Request For Inspection: Ain Tsila Development Main EPC Contract A-CNT-CON-000-00282Dokument1 SeiteRequest For Inspection: Ain Tsila Development Main EPC Contract A-CNT-CON-000-00282ZaidiNoch keine Bewertungen
- Christopher Hall@usdoj GovDokument2 SeitenChristopher Hall@usdoj GovEquality Case FilesNoch keine Bewertungen
- Concept Note ALACDokument4 SeitenConcept Note ALACdheereshkdwivediNoch keine Bewertungen
- DarapelDokument2 SeitenDarapelChristian ChetcutiNoch keine Bewertungen
- Sex Trafficking Statistics 2022 Worldwide (Bedbible - Com Reveals)Dokument4 SeitenSex Trafficking Statistics 2022 Worldwide (Bedbible - Com Reveals)PR.comNoch keine Bewertungen
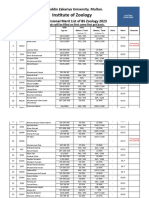
- 5953-6th Merit List BS Zool 31-8-2023Dokument22 Seiten5953-6th Merit List BS Zool 31-8-2023Muhammad AttiqNoch keine Bewertungen
- Issues in EducationDokument15 SeitenIssues in EducationChinie DomingoNoch keine Bewertungen
- Barandon Vs FerrerDokument3 SeitenBarandon Vs FerrerCorina Jane Antiga100% (1)
- Presidential Decree No. 1829, S. 1981 - Official Gazette of The Republic of The PhilippinesDokument4 SeitenPresidential Decree No. 1829, S. 1981 - Official Gazette of The Republic of The PhilippinesXean Min KuNoch keine Bewertungen
- Historical Background of The PNPDokument1 SeiteHistorical Background of The PNPGloria AsuncionNoch keine Bewertungen
- House ReceiptDokument1 SeiteHouse ReceiptArunNoch keine Bewertungen
- Chapter 8Dokument74 SeitenChapter 8Liyana AzizNoch keine Bewertungen
- Laura Lammasniemi - Law Dissertations - A Step-By-Step Guide-Routledge (2018)Dokument208 SeitenLaura Lammasniemi - Law Dissertations - A Step-By-Step Guide-Routledge (2018)Rina DewiNoch keine Bewertungen
- Special Proceedings RULE 74 - Utulo vs. PasionDokument2 SeitenSpecial Proceedings RULE 74 - Utulo vs. PasionChingkay Valente - Jimenez100% (1)
- Annotated BibliographyDokument27 SeitenAnnotated Bibliographyateam143100% (1)
- CD 116. Villaflor v. Summers, 41 Phil. 62 (1920)Dokument1 SeiteCD 116. Villaflor v. Summers, 41 Phil. 62 (1920)JMae MagatNoch keine Bewertungen