Das könnte Ihnen auch gefallen
- Referred Muscle Pain Basic and Clinical FindingsDokument9 SeitenReferred Muscle Pain Basic and Clinical FindingsaavalverdeNoch keine Bewertungen
- Journal On PainDokument5 SeitenJournal On PainGeevine CansinoNoch keine Bewertungen
- Chronic Pain and the BrainDokument17 SeitenChronic Pain and the BrainNicolas PintoNoch keine Bewertungen
- Old Ideas: The Specificity Theory of PainDokument8 SeitenOld Ideas: The Specificity Theory of Paingeloss23150% (2)
- Pain and NeuromatrixDokument5 SeitenPain and NeuromatrixBharathGopinathNoch keine Bewertungen
- Chronic Pain Management Riě VidebbDokument10 SeitenChronic Pain Management Riě VidebbRoPi212Noch keine Bewertungen
- The Cost of PainDokument121 SeitenThe Cost of PainDavid IrelandNoch keine Bewertungen
- Types of PainDokument5 SeitenTypes of PainmariyalqibtiyahNoch keine Bewertungen
- ClaudicationDokument6 SeitenClaudicationdvenumohanNoch keine Bewertungen
- How To (Seriously) Read A Scientific Paper - Science - AAASDokument14 SeitenHow To (Seriously) Read A Scientific Paper - Science - AAASKavisa GhoshNoch keine Bewertungen
- A Comparison of The Spatiotemporal Parameters, Kinematics, and BiomechanicsDokument13 SeitenA Comparison of The Spatiotemporal Parameters, Kinematics, and BiomechanicsLaura GuerreroNoch keine Bewertungen
- Posterior Tibialis Tendon Dysfunction (PTTD)Dokument11 SeitenPosterior Tibialis Tendon Dysfunction (PTTD)bigpawn13Noch keine Bewertungen
- Bodies in Flux: Scientific Methods for Negotiating Medical UncertaintyVon EverandBodies in Flux: Scientific Methods for Negotiating Medical UncertaintyNoch keine Bewertungen
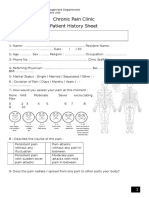
- Chronic Pain Clinic Patient History SheetDokument4 SeitenChronic Pain Clinic Patient History SheetBelal N. MahfouzNoch keine Bewertungen
- Basic Mulligan, Indikasi Dan Kontrakindikasi: Fitri Yani, M.FisDokument10 SeitenBasic Mulligan, Indikasi Dan Kontrakindikasi: Fitri Yani, M.Fisrisa tifaNoch keine Bewertungen
- Balance and Vestibular Rehabilitation KitDokument9 SeitenBalance and Vestibular Rehabilitation Kitmsnobody8Noch keine Bewertungen
- Platelet-Rich Plasma in Osteoarthritis Treatment: Review of Current EvidenceDokument18 SeitenPlatelet-Rich Plasma in Osteoarthritis Treatment: Review of Current EvidenceIrham KhairiNoch keine Bewertungen
- Good Vibrations - Do Electric Massagers WorkDokument12 SeitenGood Vibrations - Do Electric Massagers WorkMiodrag MladenovicNoch keine Bewertungen
- Biomechanics: Dr. Jewelson M. SantosDokument29 SeitenBiomechanics: Dr. Jewelson M. SantosJewelson SantosNoch keine Bewertungen
- Alpine Skiing Injuries 2018Dokument133 SeitenAlpine Skiing Injuries 2018Mariana Toledo100% (1)
- Molecular and Cellular Aspects of Muscle Function: Proceedings of the 28th International Congress of Physiological Sciences Budapest 1980, (including the proceedings of the satellite symposium on Membrane Control of Skeletal Muscle Function)Von EverandMolecular and Cellular Aspects of Muscle Function: Proceedings of the 28th International Congress of Physiological Sciences Budapest 1980, (including the proceedings of the satellite symposium on Membrane Control of Skeletal Muscle Function)E. VargaNoch keine Bewertungen
- History of PainDokument25 SeitenHistory of Paingabitor100% (1)
- Models and Mechanisms of Hyperalgesia and AllodyniaDokument52 SeitenModels and Mechanisms of Hyperalgesia and AllodyniaKarina Wibowo100% (1)
- The Mindful Body. A Prolegomenon To Future Work in Medical AnthropologyDokument37 SeitenThe Mindful Body. A Prolegomenon To Future Work in Medical AnthropologyLorena FernandezNoch keine Bewertungen
- Bio Mechanics and Motor Control of Human Movement 4editionDokument13 SeitenBio Mechanics and Motor Control of Human Movement 4editionStanko.Stuhec8307100% (2)
- Injury-Free Small FileDokument65 SeitenInjury-Free Small FileGeorge PNFNoch keine Bewertungen
- Phasic Activity of Intrinsic Muscles of The FootDokument14 SeitenPhasic Activity of Intrinsic Muscles of The FootpetcudanielNoch keine Bewertungen
- The Foot Strength Plan Healthy Feet, The Truth About Orthotics, and More (Dombroski PHD, Colin)Dokument94 SeitenThe Foot Strength Plan Healthy Feet, The Truth About Orthotics, and More (Dombroski PHD, Colin)CLOSING GENERATIONSNoch keine Bewertungen
- Pain Scale For Plantar FasciiitsDokument6 SeitenPain Scale For Plantar FasciiitsAnna HipNoch keine Bewertungen
- A Patients Guide To Plantar Fasciitis Heel PainDokument4 SeitenA Patients Guide To Plantar Fasciitis Heel PainJacobfranNoch keine Bewertungen
- Levine - Rehabilitation After Total Hip and Knee ArthroplastyDokument6 SeitenLevine - Rehabilitation After Total Hip and Knee Arthroplastyma_zinha_22Noch keine Bewertungen
- Warm-Up Reduces Delayed-Onset Muscle Soreness But Cool-Down Does Not A Randomised Controlled TrialDokument6 SeitenWarm-Up Reduces Delayed-Onset Muscle Soreness But Cool-Down Does Not A Randomised Controlled TrialMyra AshilaNoch keine Bewertungen
- Neuroplasticity: Implications For RehabilitationDokument28 SeitenNeuroplasticity: Implications For RehabilitationOmar Duran CastroNoch keine Bewertungen
- Module 2 Introduction To SPSS - WordDokument17 SeitenModule 2 Introduction To SPSS - WordJordine UmayamNoch keine Bewertungen
- Cervicovestibular Rehabilitation in Sport-Related Concussion - A Randomised Controlled TrialDokument7 SeitenCervicovestibular Rehabilitation in Sport-Related Concussion - A Randomised Controlled TrialhilmikamelNoch keine Bewertungen
- Ultrasound TherapyDokument3 SeitenUltrasound Therapyليلى مسلمة100% (1)
- Meralgia ParestheticaDokument22 SeitenMeralgia ParestheticaWahyu Tri KusprasetyoNoch keine Bewertungen
- Dynamic biomechanics of normal foot and ankle during walking and runningDokument11 SeitenDynamic biomechanics of normal foot and ankle during walking and runningPedro M. BorgesNoch keine Bewertungen
- Manual Therapy: Jo Nijs, Enrique Lluch Girb Es, Mari Lundberg, Anneleen Mal Iet, Michele SterlingDokument5 SeitenManual Therapy: Jo Nijs, Enrique Lluch Girb Es, Mari Lundberg, Anneleen Mal Iet, Michele SterlingCentro Integral KndNoch keine Bewertungen
- Scientific RepresentationDokument90 SeitenScientific RepresentationJuan Antonio SanchezNoch keine Bewertungen
- Myofascial Release for Piriformis MyalgiaDokument14 SeitenMyofascial Release for Piriformis MyalgiaApoorvNoch keine Bewertungen
- Cautionary Tales PDFDokument32 SeitenCautionary Tales PDFAfreenZaraNoch keine Bewertungen
- IOC World Conference On Prevention of Injury and Illness in Sport - April 2014 - PresentationDokument80 SeitenIOC World Conference On Prevention of Injury and Illness in Sport - April 2014 - PresentationGogy MarkNoch keine Bewertungen
- Common Causes of Forefoot PainDokument14 SeitenCommon Causes of Forefoot PainAdvanced PhysiotherapyNoch keine Bewertungen
- Butler's Neuromobilizations Combined With Proprioceptive Neuromuscular Facilitation Are Effective in Reducing of Upper Limb Sensory in Late-Stage Stroke Subjects: A Three-Group Randomized TrialDokument12 SeitenButler's Neuromobilizations Combined With Proprioceptive Neuromuscular Facilitation Are Effective in Reducing of Upper Limb Sensory in Late-Stage Stroke Subjects: A Three-Group Randomized TrialCarmen Menaya FernandezNoch keine Bewertungen
- Tennis Elbow JOSPT ArticleDokument11 SeitenTennis Elbow JOSPT ArticleHasan RahmanNoch keine Bewertungen
- MSK Us ProtocolsDokument40 SeitenMSK Us Protocolsjamir59Noch keine Bewertungen
- Medial Epicondylitis (Golfer's Elbow) - Shoulder & Elbow - OrthobulletsDokument8 SeitenMedial Epicondylitis (Golfer's Elbow) - Shoulder & Elbow - OrthobulletsSylvia GraceNoch keine Bewertungen
- UKA-John Kiely PeriodizationDokument14 SeitenUKA-John Kiely PeriodizationFagaras MoniNoch keine Bewertungen
- Presented by Yasha Ali Bangash & Pashmina Khan DPT Batch Ii Semester VDokument20 SeitenPresented by Yasha Ali Bangash & Pashmina Khan DPT Batch Ii Semester VAngelic khanNoch keine Bewertungen
- Movement Impairment and Low Back Pain Thesis SwedenDokument100 SeitenMovement Impairment and Low Back Pain Thesis SwedenwernsickleNoch keine Bewertungen
- Bone Structure MusculoskeletalDokument20 SeitenBone Structure MusculoskeletalLM MysNoch keine Bewertungen
- HumanBody - 3d Model and AnalysisDokument407 SeitenHumanBody - 3d Model and Analysissssq1Noch keine Bewertungen
- An Appreciation of Sherrington's "The Integrative Action of The Nervous System"Dokument8 SeitenAn Appreciation of Sherrington's "The Integrative Action of The Nervous System"saswepakNoch keine Bewertungen
- ISPRM Online Training Course On ESWT in PRM - Module 1Dokument94 SeitenISPRM Online Training Course On ESWT in PRM - Module 1zhangpeng100% (1)
- A Classification of Chronic Pain For ICD 11Dokument6 SeitenA Classification of Chronic Pain For ICD 11Andreas AdiwinataNoch keine Bewertungen
- Treatment of Tendinopathy What Works, What Does Not, and What Is On The Horizon PDFDokument16 SeitenTreatment of Tendinopathy What Works, What Does Not, and What Is On The Horizon PDFFranciscoJavierRoblesNoch keine Bewertungen
- Chapter 12Dokument21 SeitenChapter 12Suganthi AnbazhaganNoch keine Bewertungen
- Facts About The Hand-Off Communications ProjectDokument2 SeitenFacts About The Hand-Off Communications ProjectMukhlish MudaNoch keine Bewertungen
- Cutting, Clamping and Retracting Surgical InstrumentsDokument77 SeitenCutting, Clamping and Retracting Surgical InstrumentsAndrea Pugh0% (1)
- PETUNJUK KHUSUS PILIHAN GANDADokument12 SeitenPETUNJUK KHUSUS PILIHAN GANDARindah Tiara SariNoch keine Bewertungen
- Slipped Disc Syndrome ExplainedDokument9 SeitenSlipped Disc Syndrome ExplainedAndrei MarinNoch keine Bewertungen
- KaoshikiiDokument24 SeitenKaoshikiiapi-238078813Noch keine Bewertungen
- Thames Valley Y-Site Intravenous Drugs Compatibility ChartDokument2 SeitenThames Valley Y-Site Intravenous Drugs Compatibility ChartА. СосорбарамNoch keine Bewertungen
- Protein Energy Malnutrition - MedscapeDokument14 SeitenProtein Energy Malnutrition - MedscapeGesa Syauqi HumairaNoch keine Bewertungen
- Medical Gas Pipeline SystemsDokument218 SeitenMedical Gas Pipeline Systemsmedo2005100% (10)
- 1 Manufacture: A Typical Analysis of Commercial Chlorosulfonic Acid Would Be AsDokument6 Seiten1 Manufacture: A Typical Analysis of Commercial Chlorosulfonic Acid Would Be Asapi-19738746Noch keine Bewertungen
- Beauty Parlour 3 LakhDokument6 SeitenBeauty Parlour 3 Lakhvijay100% (1)
- Pulsion Work Booklet: Bucarest Hemodynamic Monitoring WorkshopDokument43 SeitenPulsion Work Booklet: Bucarest Hemodynamic Monitoring WorkshopghuoiNoch keine Bewertungen
- Omega 85Dokument11 SeitenOmega 85soorajssNoch keine Bewertungen
- Interventions With PneumoniaDokument2 SeitenInterventions With PneumoniaAnonymous qemC1CybLNoch keine Bewertungen
- FDA warns against Wendy's durian candy after bacteria discoveryDokument2 SeitenFDA warns against Wendy's durian candy after bacteria discoveryDesa RefuerzoNoch keine Bewertungen
- Viral Hepatitis B: Guide to Prevention and TreatmentDokument27 SeitenViral Hepatitis B: Guide to Prevention and TreatmentlailashivaNoch keine Bewertungen
- 50 Compare and ContrastDokument6 Seiten50 Compare and ContrastVeeradri SimhadriNoch keine Bewertungen
- EHealthDokument14 SeitenEHealthgomezt888Noch keine Bewertungen
- Guideline Evolution for Diagnosis and Management of DengueDokument35 SeitenGuideline Evolution for Diagnosis and Management of DengueFrinciaNoch keine Bewertungen
- Hospital AdministrationDokument25 SeitenHospital AdministrationKaushik Kansara67% (3)
- Head-To-Toe Physical Assessment Assessment Actual Findings Analysis Skin and NailsDokument8 SeitenHead-To-Toe Physical Assessment Assessment Actual Findings Analysis Skin and NailsKristen Leigh MarianoNoch keine Bewertungen
- Inside ChiropracticDokument275 SeitenInside ChiropracticDanielNoch keine Bewertungen
- Overview and Treatment Option: SkizofreniaDokument8 SeitenOverview and Treatment Option: SkizofreniaEvi LoNoch keine Bewertungen
- Bacterial Contamination in Blood Transfusion - Factors, PathogenesisDokument4 SeitenBacterial Contamination in Blood Transfusion - Factors, PathogenesisjunaidiabdhalimNoch keine Bewertungen
- HA 535 - Assignment Two Instruction - Coding Sheet Summary Table ExampleDokument2 SeitenHA 535 - Assignment Two Instruction - Coding Sheet Summary Table ExampleEsteban García EcheverryNoch keine Bewertungen
- Bio InvestDokument16 SeitenBio InvestVishakha GuptA100% (4)
- D S T E I B D B V: Esirable Pecifications For Otal Rror, Mprecision, and Ias, Erived From Iologic AriationDokument14 SeitenD S T E I B D B V: Esirable Pecifications For Otal Rror, Mprecision, and Ias, Erived From Iologic Ariationlaboratorium rsud jatipadangNoch keine Bewertungen
- Phimosis 5 PDFDokument4 SeitenPhimosis 5 PDFNurul YaqinNoch keine Bewertungen
- Urinary CatheterizationDokument11 SeitenUrinary CatheterizationPamDavidGabrielNoch keine Bewertungen
- Renal impairment and dexketoprofen pharmacokineticsDokument2 SeitenRenal impairment and dexketoprofen pharmacokineticsMaria UlfaNoch keine Bewertungen