Das könnte Ihnen auch gefallen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Substance Abuse Counseling Complete 5th EditionDokument379 SeitenSubstance Abuse Counseling Complete 5th Editionnintendoagekid86% (59)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (894)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- Bartending Written ExamDokument5 SeitenBartending Written ExamEmerson Cruz100% (3)
- Non-Alcoholic Beer-A New Industrial ProcessDokument10 SeitenNon-Alcoholic Beer-A New Industrial ProcessTrysh IoanaNoch keine Bewertungen
- ZQZQZ Qz0Zq Z0M0Z Qz0Zq ZQZQZ: Dating For Cs MajorsDokument19 SeitenZQZQZ Qz0Zq Z0M0Z Qz0Zq ZQZQZ: Dating For Cs MajorspeterNoch keine Bewertungen
- Maximizing Value from Tomato Processing WasteDokument22 SeitenMaximizing Value from Tomato Processing Wastefernando MurciaNoch keine Bewertungen
- Widening of Pat Sectors - Distillery PDFDokument45 SeitenWidening of Pat Sectors - Distillery PDFVIVEKNoch keine Bewertungen
- Report On Indian Beverage IndustryDokument19 SeitenReport On Indian Beverage IndustryAvinash BulaniNoch keine Bewertungen
- Law - Case Unit 6Dokument7 SeitenLaw - Case Unit 6Nhi Nguyễn YếnNoch keine Bewertungen
- Hosts UmbrellaDokument1 SeiteHosts UmbrellaFabsor SoralNoch keine Bewertungen
- Regiao Prelimbica Cocaina Preferencia LugarDokument8 SeitenRegiao Prelimbica Cocaina Preferencia LugarIron ChavesNoch keine Bewertungen
- Morfina Rna MensageiroDokument7 SeitenMorfina Rna MensageiroIron ChavesNoch keine Bewertungen
- Glutamato X AlzheimerDokument9 SeitenGlutamato X AlzheimerIron ChavesNoch keine Bewertungen
- Receptores de Aspartato X MemoriaDokument20 SeitenReceptores de Aspartato X MemoriaIron ChavesNoch keine Bewertungen
- Dopamina Acumbens AutoadministraçãoDokument10 SeitenDopamina Acumbens AutoadministraçãoIron ChavesNoch keine Bewertungen
- Plantas CoginiçaoDokument15 SeitenPlantas CoginiçaoIron ChavesNoch keine Bewertungen
- Receptores Gaba B X EncefaloDokument12 SeitenReceptores Gaba B X EncefaloIron ChavesNoch keine Bewertungen
- Planta Amazonia AnticolinoesteraseDokument6 SeitenPlanta Amazonia AnticolinoesteraseIron ChavesNoch keine Bewertungen
- Histamina X AlzheimerDokument7 SeitenHistamina X AlzheimerIron ChavesNoch keine Bewertungen
- Dependencia Morfina BozarthDokument11 SeitenDependencia Morfina BozarthIron ChavesNoch keine Bewertungen
- Eu Eu Mesmo e BrandaoDokument7 SeitenEu Eu Mesmo e BrandaoIron ChavesNoch keine Bewertungen
- Cronobiologia GeneticaDokument8 SeitenCronobiologia GeneticaIron ChavesNoch keine Bewertungen
- Delta 9 THC Atv N AcumbensDokument6 SeitenDelta 9 THC Atv N AcumbensIron ChavesNoch keine Bewertungen
- Alostasia Amigidala AnsiedadeDokument12 SeitenAlostasia Amigidala AnsiedadeIron ChavesNoch keine Bewertungen
- Alzheimer Modelos AnimaisDokument13 SeitenAlzheimer Modelos AnimaisIron ChavesNoch keine Bewertungen
- Alcool Naltrexona Nucelo AcumbensDokument4 SeitenAlcool Naltrexona Nucelo AcumbensIron ChavesNoch keine Bewertungen
- Antagonisa Alfa 2 X MemoriaDokument16 SeitenAntagonisa Alfa 2 X MemoriaIron ChavesNoch keine Bewertungen
- Agonistas Nicotona X CatecolaminasDokument6 SeitenAgonistas Nicotona X CatecolaminasIron ChavesNoch keine Bewertungen
- A Turma Do BrandaoDokument8 SeitenA Turma Do BrandaoIron ChavesNoch keine Bewertungen
- 222Dokument2 Seiten222Iron ChavesNoch keine Bewertungen
- 222Dokument2 Seiten222Iron ChavesNoch keine Bewertungen
- 111Dokument2 Seiten111Iron ChavesNoch keine Bewertungen
- 111Dokument2 Seiten111Iron ChavesNoch keine Bewertungen
- A Models Guide To Healthy EatingDokument5 SeitenA Models Guide To Healthy EatingIamaBillionaireNoch keine Bewertungen
- Sample Data Alcoholic Drinks BeerDokument1.633 SeitenSample Data Alcoholic Drinks BeerNere Niz ChavezNoch keine Bewertungen
- UNLV Syllabus Spirits 362 Summer 2014Dokument9 SeitenUNLV Syllabus Spirits 362 Summer 2014kevinNoch keine Bewertungen
- Does Alcohol Lower Testosterone? What You MUST KnowDokument4 SeitenDoes Alcohol Lower Testosterone? What You MUST KnowJakeNoch keine Bewertungen
- 3040010Dokument44 Seiten3040010Mark Anthony CaroNoch keine Bewertungen
- The Rise of Wine for the MassesDokument38 SeitenThe Rise of Wine for the MassesAnjali SharmaNoch keine Bewertungen
- Classification of Drinks 2206 and 2208 - Majority Test ProposalDokument1 SeiteClassification of Drinks 2206 and 2208 - Majority Test ProposalFulki Ghilman HadiansyahNoch keine Bewertungen
- Anglican Priesthood in South AfricaDokument50 SeitenAnglican Priesthood in South AfricaJoe BlowNoch keine Bewertungen
- Moonlight & Roses PDFDokument63 SeitenMoonlight & Roses PDFTitu A FaNoch keine Bewertungen
- Ethical Issues in Automobile IndustryDokument13 SeitenEthical Issues in Automobile Industrybabubothal0% (1)
- Chapter 4 BeverageDokument48 SeitenChapter 4 BeverageDarlene Mae HumbeNoch keine Bewertungen
- CHAPTER 1.2 Alcoholic BeveragesDokument58 SeitenCHAPTER 1.2 Alcoholic BeveragesFaraiyzNoch keine Bewertungen
- Case Study 19 409 1Dokument4 SeitenCase Study 19 409 1api-606957005Noch keine Bewertungen
- A Brief History of The CocktailDokument3 SeitenA Brief History of The CocktailChiritoiu Tiberiu100% (1)
- Spirits and LiqueursDokument4 SeitenSpirits and LiqueursSuchitra GopiNoch keine Bewertungen
- Cordova Public College Bar & Beverage SyllabusDokument11 SeitenCordova Public College Bar & Beverage SyllabusShammica Pacaldo DicoNoch keine Bewertungen
- Lab Report Fermentation DoneDokument3 SeitenLab Report Fermentation DoneBlank BlankNoch keine Bewertungen
- GB 2762.2012 Maximum Levels of Contaminants in Foods (Eng)Dokument19 SeitenGB 2762.2012 Maximum Levels of Contaminants in Foods (Eng)Đăng LưuNoch keine Bewertungen
- Beverage Service Techniques & Styles GuideDokument28 SeitenBeverage Service Techniques & Styles GuideMICKEY CALADIAONoch keine Bewertungen
- Food Categorization CodeDokument7 SeitenFood Categorization CodejainshinesNoch keine Bewertungen
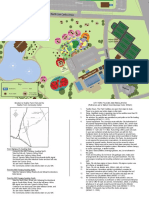
- Heather Farm Park Picnic Table BrochureDokument2 SeitenHeather Farm Park Picnic Table Brochuresdivya02Noch keine Bewertungen
- Food and Beverage ServiceDokument9 SeitenFood and Beverage ServiceManolo Solano100% (1)