Das könnte Ihnen auch gefallen
- Acute Gastritis CPG FINALDokument5 SeitenAcute Gastritis CPG FINALkimadlo656Noch keine Bewertungen
- Admit OrdersDokument2 SeitenAdmit OrdersTariq Niaz Ahmad, MDNoch keine Bewertungen
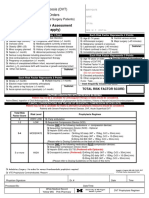
- VTE Risk AssessmentDokument2 SeitenVTE Risk AssessmentpriyopanjiNoch keine Bewertungen
- Aripiprazole AbilifyDokument2 SeitenAripiprazole AbilifyKristi Wray100% (2)
- Orthopedic Inpatient Protocols: A Guide to Orthopedic Inpatient RoundingVon EverandOrthopedic Inpatient Protocols: A Guide to Orthopedic Inpatient RoundingNoch keine Bewertungen
- Fluoxetine Duloxetine SertralineDokument7 SeitenFluoxetine Duloxetine SertralineReneé Camille100% (1)
- General Surgery Admission Order Set - Sample Template: Code StatusDokument4 SeitenGeneral Surgery Admission Order Set - Sample Template: Code StatusEricka SwordNoch keine Bewertungen
- Clinical Pathway - Stroke Without Thrombolytic TherapyDokument4 SeitenClinical Pathway - Stroke Without Thrombolytic TherapysiusiuwidyantoNoch keine Bewertungen
- Cadiac Surgery Vascular SurgeryDokument12 SeitenCadiac Surgery Vascular SurgeryRaJeev K SookunNoch keine Bewertungen
- Cardene IV Order SetDokument2 SeitenCardene IV Order SetJoe McCoyNoch keine Bewertungen
- Purpose: CVA (Stroke) Patients (Ischemic and Hemorrhagic), Management ofDokument4 SeitenPurpose: CVA (Stroke) Patients (Ischemic and Hemorrhagic), Management ofRoxanne AlvarezNoch keine Bewertungen
- Nursing Module For Brain StrokeDokument27 SeitenNursing Module For Brain StrokeziadabiakarNoch keine Bewertungen
- Practice Midterm Test.Dokument16 SeitenPractice Midterm Test.Marku LeeNoch keine Bewertungen
- Miami Dade College Care Plan ModelDokument11 SeitenMiami Dade College Care Plan ModelllubicabarkovicNoch keine Bewertungen
- ICU Admission Orders Page 1 of 5Dokument5 SeitenICU Admission Orders Page 1 of 5ramzicard943Noch keine Bewertungen
- CCU HandoverDokument9 SeitenCCU Handoverapi-192342497Noch keine Bewertungen
- Thrombosis Risk Factor Assessment (Choose All That Apply) : Deep Vein Thrombosis (DVT) Prophylaxis OrdersDokument2 SeitenThrombosis Risk Factor Assessment (Choose All That Apply) : Deep Vein Thrombosis (DVT) Prophylaxis OrdersPutu Gizha Satrya GautamaNoch keine Bewertungen
- Severe TBI 2017Dokument18 SeitenSevere TBI 2017DM internaNoch keine Bewertungen
- Post Op CABG OrdersDokument4 SeitenPost Op CABG OrdersMaria Nadia MihalikNoch keine Bewertungen
- 16464-Article Text-54657-1-10-20170124Dokument4 Seiten16464-Article Text-54657-1-10-20170124Aashish KalikaNoch keine Bewertungen
- Total Hip and Knee ReplacementsDokument57 SeitenTotal Hip and Knee ReplacementsBryndenNoch keine Bewertungen
- Anemia-Careplan For AdultDokument29 SeitenAnemia-Careplan For AdultdjbhetaNoch keine Bewertungen
- Acute Stroke ManagementDokument8 SeitenAcute Stroke ManagementГурам ЧахвадзеNoch keine Bewertungen
- Post-Op Orders - Reginald W. Martin, M.DDokument2 SeitenPost-Op Orders - Reginald W. Martin, M.DIbrahim AlmohiniNoch keine Bewertungen
- Drug Study AdalatDokument4 SeitenDrug Study AdalatLea CelestialNoch keine Bewertungen
- Problem 2Dokument9 SeitenProblem 2Chan Myae NaingNoch keine Bewertungen
- Client Information Sheet (CIS)Dokument10 SeitenClient Information Sheet (CIS)Christine RombawaNoch keine Bewertungen
- A I - E M: Drenal Nsufficiency Mergency AnagementDokument12 SeitenA I - E M: Drenal Nsufficiency Mergency AnagementCaity YoungNoch keine Bewertungen
- Medication FlashcardsDokument10 SeitenMedication FlashcardsSilvio PerezNoch keine Bewertungen
- Medically Compromised PaftientsDokument21 SeitenMedically Compromised PaftientsLedjon KaciNoch keine Bewertungen
- Pediatric Acute Sepsis: Physician'S OrdersDokument4 SeitenPediatric Acute Sepsis: Physician'S OrdersSughosh MitraNoch keine Bewertungen
- Apixaban Eliquis MonographDokument14 SeitenApixaban Eliquis MonographTran Minh NgocNoch keine Bewertungen
- Nursing Care PlansDokument11 SeitenNursing Care PlansBryan Neil GarmaNoch keine Bewertungen
- Doctor's OrdersDokument6 SeitenDoctor's OrdersKryza Dale Bunado BaticanNoch keine Bewertungen
- Admission OrdersDokument3 SeitenAdmission Ordersoyim sNoch keine Bewertungen
- Pharmacology-Final Na JudDokument17 SeitenPharmacology-Final Na JudDizerine Mirafuentes RolidaNoch keine Bewertungen
- COVID-19 Protocol KGMU Version 6.0 17-4-21Dokument34 SeitenCOVID-19 Protocol KGMU Version 6.0 17-4-21Kirtivaan MishraNoch keine Bewertungen
- Grave's Diseases ManagementDokument18 SeitenGrave's Diseases ManagementHidvardNoch keine Bewertungen
- Volume 2 GDVs and More - Rev1 Ed6jvjDokument39 SeitenVolume 2 GDVs and More - Rev1 Ed6jvjErhan ErtuçNoch keine Bewertungen
- Traumatic Brain Injury 2023Dokument17 SeitenTraumatic Brain Injury 2023Fernando Martinez AguilarNoch keine Bewertungen
- IV Iron Orders Outpatient 11.2018 PDFDokument1 SeiteIV Iron Orders Outpatient 11.2018 PDFMuhammad SaeedNoch keine Bewertungen
- MRCP Part 1Dokument38 SeitenMRCP Part 1走过一些路Noch keine Bewertungen
- Ventura County Medical Center: Mi Thrombolysis, Management ofDokument3 SeitenVentura County Medical Center: Mi Thrombolysis, Management ofblackcat657Noch keine Bewertungen
- Acs 11 190524110746Dokument46 SeitenAcs 11 190524110746Obakeng MandaNoch keine Bewertungen
- Medical Toxicology Part 2Dokument68 SeitenMedical Toxicology Part 2chuck kieNoch keine Bewertungen
- Drug Monograph XareltoDokument2 SeitenDrug Monograph XareltoBenNoch keine Bewertungen
- 508 Medication PreAssignmentDokument9 Seiten508 Medication PreAssignmentMikeNoch keine Bewertungen
- Lisinopril, TAB: Generic Name of Medication: Brand/trade Name of MedicationDokument6 SeitenLisinopril, TAB: Generic Name of Medication: Brand/trade Name of MedicationCliff by the seaNoch keine Bewertungen
- Case Study, Chapter 54, Management of Patients With Kidney DisordersDokument4 SeitenCase Study, Chapter 54, Management of Patients With Kidney DisordersInsieNoch keine Bewertungen
- Inclusion Criteria:: Urinary Tract Infection Care MapDokument9 SeitenInclusion Criteria:: Urinary Tract Infection Care MapMoh. H.AlObaidyNoch keine Bewertungen
- Stroke by Dr. Amit RoyDokument32 SeitenStroke by Dr. Amit RoyDr Sutanwi DasNoch keine Bewertungen
- Acute Coronary Syndrome (ACS) : Basic Principles For ACSDokument4 SeitenAcute Coronary Syndrome (ACS) : Basic Principles For ACSRendra DananjayaNoch keine Bewertungen
- PRE ANAESTHETIC ASSESSMENT New 1Dokument41 SeitenPRE ANAESTHETIC ASSESSMENT New 1lokeswara reddyNoch keine Bewertungen
- Laparoscopic AdrenalectomyDokument21 SeitenLaparoscopic AdrenalectomyHu EyongNoch keine Bewertungen
- Clonidine Hydrochloride (Drug Study)Dokument2 SeitenClonidine Hydrochloride (Drug Study)Franz.thenurse688875% (4)
- Acute Myocardial Infarction: Recognition and AssessmentDokument7 SeitenAcute Myocardial Infarction: Recognition and AssessmentHasnainKhimjiNoch keine Bewertungen
- Discharge Advice After Your Coronary Angiogram, Angioplasty or Stent Insertion (PCI)Dokument16 SeitenDischarge Advice After Your Coronary Angiogram, Angioplasty or Stent Insertion (PCI)Nazmul Alam FarukiNoch keine Bewertungen
- Drugs ACSDokument5 SeitenDrugs ACSGilbert NeahNoch keine Bewertungen
- 6 - Fahad Class 6 Cardiac AnesthesiaDokument18 Seiten6 - Fahad Class 6 Cardiac AnesthesiaOne ClickNoch keine Bewertungen
- IFM+Toolkit+Table+of+Contents v19Dokument13 SeitenIFM+Toolkit+Table+of+Contents v19khaled dewanNoch keine Bewertungen
- Open Heart Surgery CaabgDokument6 SeitenOpen Heart Surgery CaabgGopi KrishnanNoch keine Bewertungen
- 2017 Spine CPT Code Changes: Kim Pollock, RN, MBA, CPC, CMDPDokument4 Seiten2017 Spine CPT Code Changes: Kim Pollock, RN, MBA, CPC, CMDPZakariaAwaludinNoch keine Bewertungen
- Icu-Related Dysphagia Epidemiology, Pathophysiology, Diagnostics and TreatmentDokument6 SeitenIcu-Related Dysphagia Epidemiology, Pathophysiology, Diagnostics and TreatmentLuis De jesus SolanoNoch keine Bewertungen
- LAS For Summative Assessment (Written Work Performance Task)Dokument2 SeitenLAS For Summative Assessment (Written Work Performance Task)Angel Dela CruzNoch keine Bewertungen
- All India Institute of Medical Sciences, Nagpur Result NotificationDokument4 SeitenAll India Institute of Medical Sciences, Nagpur Result NotificationNayan ChaudhariNoch keine Bewertungen
- Acosta, Joyce Ara T. Week 7 & 8 Drug StudyDokument11 SeitenAcosta, Joyce Ara T. Week 7 & 8 Drug StudyJoyce Ara Tumbaga AcostaNoch keine Bewertungen
- Final PhysicalDokument409 SeitenFinal PhysicalAbhishiktaAbhiNoch keine Bewertungen
- Case Obsos SellyDokument24 SeitenCase Obsos SellyDwi CahyaNoch keine Bewertungen
- MSE DepressionDokument3 SeitenMSE DepressionSam Raven AndresNoch keine Bewertungen
- Dr. Mohammed Shahedur Rahman Khan Bronchial Asthma Management Aspects - Current and FutureDokument32 SeitenDr. Mohammed Shahedur Rahman Khan Bronchial Asthma Management Aspects - Current and FutureShahadat Hossain BabuNoch keine Bewertungen
- Somniferous Poisons: DR M. Malleswari Asso. Prof Nri Medical CollegeDokument58 SeitenSomniferous Poisons: DR M. Malleswari Asso. Prof Nri Medical CollegeSudheera RachamallaNoch keine Bewertungen
- White Blood Cells TugasDokument6 SeitenWhite Blood Cells TugasanisaNoch keine Bewertungen
- Medical DeviceDokument45 SeitenMedical DevicewardaddyNoch keine Bewertungen
- Asthma Treatment GuidlineDokument56 SeitenAsthma Treatment GuidlineEsther OdumanyeNoch keine Bewertungen
- Cardiac GlycosidesDokument5 SeitenCardiac Glycosidesapi-347182709100% (1)
- 4 Circulation Disorders PDFDokument69 Seiten4 Circulation Disorders PDFSetiawan SukmadjaNoch keine Bewertungen
- Renal Function TestsDokument23 SeitenRenal Function TestsKer YehunNoch keine Bewertungen
- India's 1 Health Management LabDokument14 SeitenIndia's 1 Health Management LabAjay Kumar dasNoch keine Bewertungen
- Hematology LaboratoryDokument3 SeitenHematology LaboratoryDee GeeNoch keine Bewertungen
- Sahi ExportDokument8 SeitenSahi ExportHeena ChoudharyNoch keine Bewertungen
- Muscular System FunctionDokument2 SeitenMuscular System FunctionLachlan PalmerNoch keine Bewertungen
- Therapeutic Conference: FacilitatorsDokument4 SeitenTherapeutic Conference: FacilitatorsJolaine ValloNoch keine Bewertungen
- Small Pox: A Child Infected With SmallpoxDokument5 SeitenSmall Pox: A Child Infected With SmallpoxJavee_Viccent__5618Noch keine Bewertungen
- Prolapse Lumbar DiscDokument40 SeitenProlapse Lumbar DiscAlfred BantigueNoch keine Bewertungen
- A Patient of Poisoning in ICU (Ankit Jain)Dokument48 SeitenA Patient of Poisoning in ICU (Ankit Jain)SharryNoch keine Bewertungen
- Immunochemistry and BiosensorsDokument13 SeitenImmunochemistry and BiosensorsPalak AgarwalNoch keine Bewertungen
- Quiz TraumaDokument1 SeiteQuiz Traumaaqsa rehmanNoch keine Bewertungen
- Surgery Surgical Nursing Objs With AnsDokument136 SeitenSurgery Surgical Nursing Objs With AnsmintahmeshackbenjaminNoch keine Bewertungen