Das könnte Ihnen auch gefallen
- Glomerular FiltrationDokument3 SeitenGlomerular FiltrationyolandadwiooNoch keine Bewertungen
- Assignment 1 TranscultureDokument14 SeitenAssignment 1 Transcultureiqmal irfamimi100% (1)
- Hormones of The Adrenal Cortex 1-13Dokument47 SeitenHormones of The Adrenal Cortex 1-13abstabs50% (2)
- Adrenal Hormone 2018 PDFDokument66 SeitenAdrenal Hormone 2018 PDFrosyidafiaNoch keine Bewertungen
- Concepts of Community and Public Health NursingDokument9 SeitenConcepts of Community and Public Health NursingTheophilus BaidooNoch keine Bewertungen
- CPG Management of Hypertension (4th Edition)Dokument98 SeitenCPG Management of Hypertension (4th Edition)ssfdsNoch keine Bewertungen
- Urine Formation: Mohamad Ashraf IsmailDokument13 SeitenUrine Formation: Mohamad Ashraf IsmailAshraf MobyNoch keine Bewertungen
- Type 2 Diabetes Mellitus - A Review of Current TrendsDokument5 SeitenType 2 Diabetes Mellitus - A Review of Current TrendsRevivo RindaNoch keine Bewertungen
- Project B EdDokument17 SeitenProject B EdAnju VijayanNoch keine Bewertungen
- Trichomoniasis: Clinical Manifestations, Diagnosis and ManagementDokument6 SeitenTrichomoniasis: Clinical Manifestations, Diagnosis and ManagementRabecca TobingNoch keine Bewertungen
- Patofisiologi Kidney StonesDokument8 SeitenPatofisiologi Kidney StonespipitNoch keine Bewertungen
- Welcome To N.G Acharya and D.K. Maratha College: - Aditya NashteDokument5 SeitenWelcome To N.G Acharya and D.K. Maratha College: - Aditya NashteTHE ELECTRONIC SQUADNoch keine Bewertungen
- Cardiac TumorsDokument37 SeitenCardiac TumorsdadupipaNoch keine Bewertungen
- Hypertensive Renal DiseaseDokument2 SeitenHypertensive Renal DiseaseHenry KaweesaNoch keine Bewertungen
- Triglycerides and VLDL: (Increased Ra Tio of Triglyceride To Apob)Dokument20 SeitenTriglycerides and VLDL: (Increased Ra Tio of Triglyceride To Apob)Indah Pujiati DtNoch keine Bewertungen
- Liver Function Test: AssignmentDokument6 SeitenLiver Function Test: Assignmentsaud100% (2)
- Government Schemes For Senior Citizens: 1.1 Concept and DefinitionDokument16 SeitenGovernment Schemes For Senior Citizens: 1.1 Concept and DefinitionRajasekaranindia2002Noch keine Bewertungen
- Hypertension Case StudyDokument2 SeitenHypertension Case Studyapi-344630051Noch keine Bewertungen
- Assessment of Knowledge of Chronic Kidney Disease PDFDokument7 SeitenAssessment of Knowledge of Chronic Kidney Disease PDFمالك مناصرةNoch keine Bewertungen
- Coping With Stress of Family Caregivers of CancerDokument6 SeitenCoping With Stress of Family Caregivers of CancerALFIATUR RahmiNoch keine Bewertungen
- Fluid Electrolytes and Acid Base BalanceDokument108 SeitenFluid Electrolytes and Acid Base BalancesayednourNoch keine Bewertungen
- HDL Classification SlidesDokument20 SeitenHDL Classification SlidesRainolNoch keine Bewertungen
- Patients With Hypertensive Nephropathy and Chronic Kidney Disease Might Not Benefit From Strict Blood Pressure Control PDFDokument10 SeitenPatients With Hypertensive Nephropathy and Chronic Kidney Disease Might Not Benefit From Strict Blood Pressure Control PDFSayf QisthiNoch keine Bewertungen
- Policy Brief Homeless and HealthcareDokument4 SeitenPolicy Brief Homeless and Healthcareapi-239640492Noch keine Bewertungen
- Precision MedicineDokument23 SeitenPrecision MedicineLavina Jain100% (1)
- Nutr 409 Case Study 12Dokument5 SeitenNutr 409 Case Study 12api-314354953100% (2)
- 5 HypertensionDokument219 Seiten5 HypertensionRaul GascueñaNoch keine Bewertungen
- Phobias - See What Makes Some People AfraidDokument2 SeitenPhobias - See What Makes Some People Afraidbeep777Noch keine Bewertungen
- Mechanism of Urine FormationDokument5 SeitenMechanism of Urine FormationovacuteNoch keine Bewertungen
- 47Dokument2 Seiten47Gpe C. BaronNoch keine Bewertungen
- Dengue ArticleDokument16 SeitenDengue ArticleJobelAringoNuvalNoch keine Bewertungen
- SiadhDokument16 SeitenSiadhGokul Rajan100% (1)
- Psychiatric Case StudyDokument12 SeitenPsychiatric Case Studyapi-607289995Noch keine Bewertungen
- The Problem and Its BackgroundDokument46 SeitenThe Problem and Its Backgroundharoldpaulo100% (1)
- Stevens-Johnson Syndrome (SJS)Dokument27 SeitenStevens-Johnson Syndrome (SJS)Risang de ApuestoNoch keine Bewertungen
- CasestudyDokument11 SeitenCasestudyapi-272773859Noch keine Bewertungen
- Clinical Presentation, Pathologic Features, Diagnosis, and Differential Diagnosis of Chronic Lymphocytic Leukemia - UpToDateDokument23 SeitenClinical Presentation, Pathologic Features, Diagnosis, and Differential Diagnosis of Chronic Lymphocytic Leukemia - UpToDateJosé Martínez100% (1)
- Hiv Case StudyDokument2 SeitenHiv Case Studyapi-485814878Noch keine Bewertungen
- Media Impact On HealthDokument2 SeitenMedia Impact On HealthDon J AsuncionNoch keine Bewertungen
- Principles of GeriatricsDokument12 SeitenPrinciples of GeriatricsEveryday LearnerNoch keine Bewertungen
- Liver Function Test FinalDokument98 SeitenLiver Function Test FinalHussain AzharNoch keine Bewertungen
- Clinical Reasoning QuestionsDokument8 SeitenClinical Reasoning Questionsvrasiah100% (1)
- Chapter 4 Health and Illness PDFDokument10 SeitenChapter 4 Health and Illness PDFJa YaNoch keine Bewertungen
- Biochemistry of GlycoproteinDokument6 SeitenBiochemistry of GlycoproteinMahathir Mohmed100% (7)
- 05 SMRK5103 - Part 3 - IDokument45 Seiten05 SMRK5103 - Part 3 - Inursyahirahrosli100% (1)
- Mental Health Intro (HRA PRESENTATION)Dokument11 SeitenMental Health Intro (HRA PRESENTATION)John Odutemu (Lagos Psychologist)Noch keine Bewertungen
- Systemic Lupus ErythematosusDokument22 SeitenSystemic Lupus ErythematosusYaska MusaNoch keine Bewertungen
- Approach To HypertensionDokument16 SeitenApproach To HypertensionShradha KhuranaNoch keine Bewertungen
- CholeraDokument5 SeitenCholerabishnu011978Noch keine Bewertungen
- ThalassemiaDokument24 SeitenThalassemiaanimesh panda100% (1)
- Lower Urinary Tract Symptoms (LUTS)Dokument26 SeitenLower Urinary Tract Symptoms (LUTS)Ayi Abdul BasithNoch keine Bewertungen
- Esrd Ppt. - Alex (Final)Dokument109 SeitenEsrd Ppt. - Alex (Final)Shoixi ⎝⓿⏝⓿⎠Noch keine Bewertungen
- ST - Lukes Casepress.Dokument31 SeitenST - Lukes Casepress.Justin EduardoNoch keine Bewertungen
- Pain ManagementDokument20 SeitenPain ManagementLis SyuwaibatulNoch keine Bewertungen
- Acute Limb IschemiaDokument18 SeitenAcute Limb Ischemiakarl abiaadNoch keine Bewertungen
- Chapter 28 Electroconvulsive Therapy (ECT)Dokument13 SeitenChapter 28 Electroconvulsive Therapy (ECT)VikneswariNoch keine Bewertungen
- L2 Renal Blood Flow and Glomerular Filtration 2023 1.2Dokument6 SeitenL2 Renal Blood Flow and Glomerular Filtration 2023 1.2bgj9cddvxhNoch keine Bewertungen
- Urine FormationDokument49 SeitenUrine FormationMajd HusseinNoch keine Bewertungen
- Renal SystemDokument19 SeitenRenal SystemAml Sayed Elbadwie KotbNoch keine Bewertungen
- Physio Reviewer Renal To Acid BaseDokument11 SeitenPhysio Reviewer Renal To Acid BaseNicole ChanNoch keine Bewertungen
- Chronic Renal Failure: Concise Long Case ApproachDokument3 SeitenChronic Renal Failure: Concise Long Case ApproachUsman Ali AkbarNoch keine Bewertungen
- GI Bleeding Team Work - 2nd EditionDokument9 SeitenGI Bleeding Team Work - 2nd EditionUsman Ali AkbarNoch keine Bewertungen
- Polycystic Kidneys: Adult PKD: ComplicationsDokument1 SeitePolycystic Kidneys: Adult PKD: ComplicationsUsman Ali AkbarNoch keine Bewertungen
- Renal Tubular Acidosis Summary - AdjDokument1 SeiteRenal Tubular Acidosis Summary - AdjUsman Ali AkbarNoch keine Bewertungen
- Urinary Tract Infection & PyelonephritisDokument3 SeitenUrinary Tract Infection & PyelonephritisUsman Ali AkbarNoch keine Bewertungen
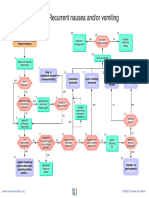
- Recurrent Nausea Andor VomitingDokument8 SeitenRecurrent Nausea Andor VomitingUsman Ali AkbarNoch keine Bewertungen
- King Khalid University Hospital Department of Obstetrics & Gyncology Course 481Dokument40 SeitenKing Khalid University Hospital Department of Obstetrics & Gyncology Course 481Usman Ali AkbarNoch keine Bewertungen
- DialysisDokument2 SeitenDialysisUsman Ali AkbarNoch keine Bewertungen
- Obstructive Airway Disease: Dr. Khalid Al-Mobaireek King Khalid University HospitalDokument53 SeitenObstructive Airway Disease: Dr. Khalid Al-Mobaireek King Khalid University HospitalUsman Ali AkbarNoch keine Bewertungen
- Anaemia in PregnancyDokument13 SeitenAnaemia in PregnancyUsman Ali AkbarNoch keine Bewertungen
- Through The Strange WindsDokument5 SeitenThrough The Strange WindsUsman Ali AkbarNoch keine Bewertungen
- Subject: Permission For Badminton Court NID, Multan: TH THDokument1 SeiteSubject: Permission For Badminton Court NID, Multan: TH THUsman Ali AkbarNoch keine Bewertungen
- DR Othman Alharbi, MBBS FRCPC Assistance Professor & Consultant Gastroenterology College of Medicine King Saud UniversityDokument18 SeitenDR Othman Alharbi, MBBS FRCPC Assistance Professor & Consultant Gastroenterology College of Medicine King Saud UniversityUsman Ali AkbarNoch keine Bewertungen
- Recurrent VomitingDokument16 SeitenRecurrent VomitingUsman Ali AkbarNoch keine Bewertungen
- GRAM NEGATIVE RODS (5) Fastidious Organisms From Animal Sources (A)Dokument1 SeiteGRAM NEGATIVE RODS (5) Fastidious Organisms From Animal Sources (A)Usman Ali AkbarNoch keine Bewertungen
- Cord ProlapseDokument2 SeitenCord ProlapseUsman Ali AkbarNoch keine Bewertungen
- Organophosphate PoisoningDokument23 SeitenOrganophosphate PoisoningUsman Ali AkbarNoch keine Bewertungen
- Alas!! EmpytinessDokument2 SeitenAlas!! EmpytinessUsman Ali AkbarNoch keine Bewertungen
- When Hope DiesDokument2 SeitenWhen Hope DiesUsman Ali AkbarNoch keine Bewertungen
- Untold Stanza... : - Nasim Alam (N-61)Dokument1 SeiteUntold Stanza... : - Nasim Alam (N-61)Usman Ali AkbarNoch keine Bewertungen
- Lect 1:: M2Pasysl21 Urinary SystemDokument4 SeitenLect 1:: M2Pasysl21 Urinary SystemUsman Ali AkbarNoch keine Bewertungen
- Death and The Mother For MergeDokument4 SeitenDeath and The Mother For MergeUsman Ali AkbarNoch keine Bewertungen
- Renal Physiology: Structure & Function of Kidneys and Urinary System, Processes and MicturitionDokument16 SeitenRenal Physiology: Structure & Function of Kidneys and Urinary System, Processes and MicturitionSufyan MirzaNoch keine Bewertungen
- Nursing Practice IvDokument24 SeitenNursing Practice IvJohn wewNoch keine Bewertungen
- Biology 1Dokument15 SeitenBiology 1maielsherif2020Noch keine Bewertungen
- Mdcat 2017Dokument52 SeitenMdcat 2017Qamar IrfanNoch keine Bewertungen
- Dialysis - Need and Types in Dialysis - 13131Dokument23 SeitenDialysis - Need and Types in Dialysis - 13131muthuNoch keine Bewertungen
- Untitled25 PDFDokument17 SeitenUntitled25 PDFElizabeth LeonNoch keine Bewertungen
- Kidney HistogenesisDokument9 SeitenKidney HistogenesisKshitija KasturiNoch keine Bewertungen
- Basic Clinical Laboratory Techniques 6Th Edition Estridge Solutions Manual Full Chapter PDFDokument60 SeitenBasic Clinical Laboratory Techniques 6Th Edition Estridge Solutions Manual Full Chapter PDFflorenceronaldoxo0100% (11)
- Renal New Growth - NCM 103 - or CaseDokument19 SeitenRenal New Growth - NCM 103 - or CasePat EnriquezNoch keine Bewertungen
- SHS.108.Lect-10 Tubular ReabsorptionDokument61 SeitenSHS.108.Lect-10 Tubular ReabsorptionAzlan YasirNoch keine Bewertungen
- Chapter 3-Coordination and ResponseDokument48 SeitenChapter 3-Coordination and ResponseShuhaida JamaludinNoch keine Bewertungen
- The Kidney - Hansel Et Al. - 1 Ed. (2016) - enDokument218 SeitenThe Kidney - Hansel Et Al. - 1 Ed. (2016) - enDuda EvangelistaNoch keine Bewertungen
- The Excretory System: Back To TopDokument10 SeitenThe Excretory System: Back To TopDANIA PURNAMANoch keine Bewertungen
- Excretory Products and Their EliminationDokument7 SeitenExcretory Products and Their EliminationKajal SinghNoch keine Bewertungen
- Complete Urinalysis and Urine Test-2Dokument34 SeitenComplete Urinalysis and Urine Test-2azuraNoch keine Bewertungen
- Renal/Genitourinary Disorders: Ncm-104 Pediatric NursingDokument56 SeitenRenal/Genitourinary Disorders: Ncm-104 Pediatric NursingCherrie FayeNoch keine Bewertungen
- H 4.2 Histology Urinary SystemDokument52 SeitenH 4.2 Histology Urinary SystemF N100% (2)
- NSEJS 2022 Question Paper With SolutionsDokument47 SeitenNSEJS 2022 Question Paper With SolutionsPRITHISH HAZRANoch keine Bewertungen
- British Biology Olympiad 2012 Round Two Question Paper: Time Allowed 1Dokument24 SeitenBritish Biology Olympiad 2012 Round Two Question Paper: Time Allowed 1Malvina YuanNoch keine Bewertungen
- EDS Multiple Choice QuestionsDokument4 SeitenEDS Multiple Choice QuestionsbalochimrankhanNoch keine Bewertungen
- Renal Physiology MCQDokument12 SeitenRenal Physiology MCQTran Dong67% (9)
- Funda SL FinalsDokument3 SeitenFunda SL FinalsKarylle Joy ValenciaNoch keine Bewertungen
- Urinary SystemDokument22 SeitenUrinary SystemGray Odyssey M.Noch keine Bewertungen
- Renal Tubular Acidosis and Management Strategies: A Narrative ReviewDokument20 SeitenRenal Tubular Acidosis and Management Strategies: A Narrative ReviewMacarena SainzNoch keine Bewertungen
- 5 Must To Know in Clinical Micros PDFDokument43 Seiten5 Must To Know in Clinical Micros PDFYelai CarveroNoch keine Bewertungen
- Biology 2nd Year - Objective Mcqs - Ali Raza - Ark PDFDokument53 SeitenBiology 2nd Year - Objective Mcqs - Ali Raza - Ark PDFAsad Mehmood100% (1)
- Physiology Paper 1 Question BankDokument8 SeitenPhysiology Paper 1 Question BankVeshalinee100% (1)
- BIOL 0200 - Lab ManualDokument38 SeitenBIOL 0200 - Lab ManualShandev IndoiNoch keine Bewertungen
- McqsDokument13 SeitenMcqsDr. Anil LandgeNoch keine Bewertungen
- Science Exclusive Sample PaperDokument12 SeitenScience Exclusive Sample PaperbadasserytechNoch keine Bewertungen
- Periodic Tales: A Cultural History of the Elements, from Arsenic to ZincVon EverandPeriodic Tales: A Cultural History of the Elements, from Arsenic to ZincBewertung: 3.5 von 5 Sternen3.5/5 (137)
- It's Elemental: The Hidden Chemistry in EverythingVon EverandIt's Elemental: The Hidden Chemistry in EverythingBewertung: 4 von 5 Sternen4/5 (10)
- The Nature of Drugs Vol. 1: History, Pharmacology, and Social ImpactVon EverandThe Nature of Drugs Vol. 1: History, Pharmacology, and Social ImpactBewertung: 5 von 5 Sternen5/5 (5)
- ICH Quality Guidelines: An Implementation GuideVon EverandICH Quality Guidelines: An Implementation GuideAndrew TeasdaleNoch keine Bewertungen
- The Regenerative Grower's Guide to Garden Amendments: Using Locally Sourced Materials to Make Mineral and Biological Extracts and FermentsVon EverandThe Regenerative Grower's Guide to Garden Amendments: Using Locally Sourced Materials to Make Mineral and Biological Extracts and FermentsBewertung: 5 von 5 Sternen5/5 (3)
- Chemistry for Breakfast: The Amazing Science of Everyday LifeVon EverandChemistry for Breakfast: The Amazing Science of Everyday LifeBewertung: 4.5 von 5 Sternen4.5/5 (14)
- Chemistry: a QuickStudy Laminated Reference GuideVon EverandChemistry: a QuickStudy Laminated Reference GuideBewertung: 5 von 5 Sternen5/5 (1)
- The Nature of Drugs Vol. 1: History, Pharmacology, and Social ImpactVon EverandThe Nature of Drugs Vol. 1: History, Pharmacology, and Social ImpactBewertung: 5 von 5 Sternen5/5 (1)
- Handbook of Formulating Dermal Applications: A Definitive Practical GuideVon EverandHandbook of Formulating Dermal Applications: A Definitive Practical GuideNoch keine Bewertungen
- Monkeys, Myths, and Molecules: Separating Fact from Fiction, and the Science of Everyday LifeVon EverandMonkeys, Myths, and Molecules: Separating Fact from Fiction, and the Science of Everyday LifeBewertung: 4 von 5 Sternen4/5 (1)
- The Production of Volatile Oils and Perfumery Plants in the United StatesVon EverandThe Production of Volatile Oils and Perfumery Plants in the United StatesNoch keine Bewertungen
- Is That a Fact?: Frauds, Quacks, and the Real Science of Everyday LifeVon EverandIs That a Fact?: Frauds, Quacks, and the Real Science of Everyday LifeBewertung: 5 von 5 Sternen5/5 (4)
- AP Chemistry Flashcards, Fourth Edition: Up-to-Date Review and PracticeVon EverandAP Chemistry Flashcards, Fourth Edition: Up-to-Date Review and PracticeNoch keine Bewertungen
- The Nature of Drugs Vol. 2: History, Pharmacology, and Social ImpactVon EverandThe Nature of Drugs Vol. 2: History, Pharmacology, and Social ImpactNoch keine Bewertungen
- Chemistry for Breakfast: The Amazing Science of Everyday LifeVon EverandChemistry for Breakfast: The Amazing Science of Everyday LifeBewertung: 4.5 von 5 Sternen4.5/5 (90)