Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5782)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (72)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Case Study About Cervical CancerDokument11 SeitenCase Study About Cervical CancerJisel-Apple Bulan100% (1)
- Nursing Care for Couples Struggling with InfertilityDokument25 SeitenNursing Care for Couples Struggling with InfertilityTiffany Joy QuiliopeNoch keine Bewertungen
- Health-8 Q2 Mod-4 Motherhood-Journey v2 PDFDokument29 SeitenHealth-8 Q2 Mod-4 Motherhood-Journey v2 PDFTricia Nicole Caguioa DoradoNoch keine Bewertungen
- Tutorial 4.5Dokument4 SeitenTutorial 4.5Rosa FinizioNoch keine Bewertungen
- Romero-Caicedo2015 Raya GuitarraDokument15 SeitenRomero-Caicedo2015 Raya GuitarraALHONDRA HORTENCIA GOMEZ SANCHEZNoch keine Bewertungen
- 7B Reproduction Test 2004Dokument2 Seiten7B Reproduction Test 2004api-3698146100% (3)
- Human Sexuality Is The Capacity To HaveDokument74 SeitenHuman Sexuality Is The Capacity To HaveKlaus AlmesNoch keine Bewertungen
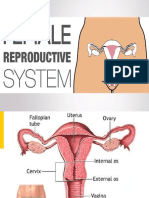
- Female Reproductive System OverviewDokument49 SeitenFemale Reproductive System OverviewJohaifha CompaniaNoch keine Bewertungen
- sCIENCE 7Dokument3 SeitensCIENCE 7Julien PitogoNoch keine Bewertungen
- REPRODUCTIVE SYSTEM REVIEWER (M and F)Dokument2 SeitenREPRODUCTIVE SYSTEM REVIEWER (M and F)Yerenica BelgoatNoch keine Bewertungen
- Performance Task 1Dokument3 SeitenPerformance Task 1Jellie May RomeroNoch keine Bewertungen
- VGO 411 Veterinary GynaecologyDokument191 SeitenVGO 411 Veterinary GynaecologyChandan PatilNoch keine Bewertungen
- ISUOG Basic Training: Examining The Uterus, Cervix, Ovaries & Adnexae: Normal FindingsDokument51 SeitenISUOG Basic Training: Examining The Uterus, Cervix, Ovaries & Adnexae: Normal FindingsDian Putri NingsihNoch keine Bewertungen
- Jurnal Kuda 1Dokument21 SeitenJurnal Kuda 1Yulistia FadhilahNoch keine Bewertungen
- 1st Summative Test in MAPEH 5Dokument3 Seiten1st Summative Test in MAPEH 5Melerose Dela Serna100% (3)
- MCN Case Presentation Group 2 1Dokument68 SeitenMCN Case Presentation Group 2 1Mary-Ann JagonobNoch keine Bewertungen
- Female Reproductive System Anatomy and PhysiologyDokument5 SeitenFemale Reproductive System Anatomy and PhysiologyIkea Balhon100% (3)
- Asetokarmin 1Dokument8 SeitenAsetokarmin 1Bank Thiti MNoch keine Bewertungen
- Graafian follicles and ovarian cystsDokument22 SeitenGraafian follicles and ovarian cystsAlemania IkakusumaNoch keine Bewertungen
- Worksheet On Human Reproduction - Grade 12Dokument27 SeitenWorksheet On Human Reproduction - Grade 12Palani G Pazhani GNoch keine Bewertungen
- Ceasarean-Case-Study NewDokument23 SeitenCeasarean-Case-Study NewPATRICIA SAN PEDRONoch keine Bewertungen
- Poultry Management Lecture2Dokument114 SeitenPoultry Management Lecture2thanh ba mat100% (1)
- Gachua Captive Breeding FinalDokument12 SeitenGachua Captive Breeding FinaljosekinNoch keine Bewertungen
- MedicalOfficer Unani 102021 182022 PDFDokument42 SeitenMedicalOfficer Unani 102021 182022 PDFbakhtiari baqavi bakhtiari baqaviNoch keine Bewertungen
- Jonathan Otto Natural Medicine SecretsDokument250 SeitenJonathan Otto Natural Medicine SecretsMax Bibi100% (5)
- Female Reproductive System QuestionsDokument264 SeitenFemale Reproductive System QuestionsrayanNoch keine Bewertungen
- Menstrual Cycle: An IntroductionDokument6 SeitenMenstrual Cycle: An IntroductionAudrie Allyson GabalesNoch keine Bewertungen
- The Endocrine SystemDokument24 SeitenThe Endocrine System속강대Noch keine Bewertungen
- Gynecologic Problems of Childhood: Anne Margrette C. VelasquezDokument46 SeitenGynecologic Problems of Childhood: Anne Margrette C. VelasquezAnne Margrette Velasquez100% (1)
- Crocodiles - Biology, Husbandry and DiseasesDokument352 SeitenCrocodiles - Biology, Husbandry and DiseasesSiva Subramanian100% (1)